

Lower partial pubicectomy for postoperative complicated posterior urethral stricture
- PMID: 37642798
- PMCID: PMC10853320
- DOI: 10.1007/s11255-023-03746-3
Lower partial pubicectomy for postoperative complicated posterior urethral stricture
Abstract
Objective: To report the experience of partial inferior pubicectomy in the treatment of complex posterior urethral stricture after trauma.
Methods: A total of 46 patients with post-traumatic posterior urethral stricture admitted to the Department of Urology of our Hospital from January 2013 to September 2021 were selected as the research objects and underwent urethroplasty (including nine patients who had failed previous perineal repair surgery and adopted partial inferior pubicectomy approach). Retrograde urethrograph (RUG) and urine flow measurement were performed at 1, 3, 12 and 18 months after operation, and follow-up was performed when necessary. The clinical data during treatment were statistically analyzed.
Results: All 46 patients underwent urethroplasty successfully, of which nine were treated with partial pubicectomy, accounting for 19.57% of the total. The causes of the disease were motor vehicle accident in 4 cases, falling collision injury in 2 cases, and rolling injury of military exercise tank in 3 cases. Among the 9 patients, 2 were children (22.22%), aged 8 and 12 years, and 7 were adults (77.78%), aged 19-44 (28.42 ± 1.56) years. Among the 9 patients, 6 had erectile dysfunction, accounting for 66.67%. The length of posterior urinary tract stenosis was (5.12 ± 0.57) cm. The operation time was (290.34 ± 12.35) min from anesthesia induction to skin closure. Five patients received 2 U blood transfusion during operation and three patients received 3 U blood transfusion after operation. The average hospital stay was 12-16 (14.24 ± 1.25) days, and the follow-up was 12-24 (18.24 ± 1.35) months. After surgery, one patient developed HIP abscess, which was successfully treated conservatively. One patient had dysuria 1 month after operation and was successfully treated by transurethral dilatation. One case had postoperative infection and recovered after intravenous administration of potent antibiotics. Cystourethrography was performed 3 months after operation, and there was no difference between patients with wide, long or short anastomotic stretch defects. All patients met the criteria for surgical success.
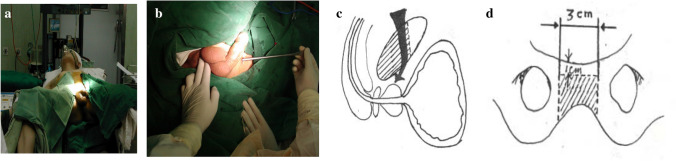
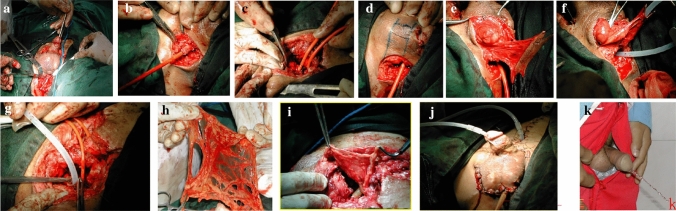
Conclusion: Partial inferior pubicectomy is a good surgical procedure for the repair of complicated posterior urethral stricture after operation. It is safe and reliable, can better display the prostatic apex and surgical field, shorten the length of reconstructed urethra, and has good postoperative effect. It has no direct or long-term effect on the stability of pelvis or bladder. However, further studies in a larger cohort of patients with complex posterior urethral strictures after repair are needed to demonstrate the specific indications for partial pubicectomy.
Keywords: Complex posterior urethral stricture; Inferior partial pubicectomy; Urethroplasty.
© 2023. The Author(s).
Conflict of interest statement
The authors declared that they have no conflicts of interest regarding this pudendal resection.
Figures

Similar articles
-
Delayed surgical repair of posttraumatic posterior urethral distraction defects in children and adolescents: long-term results.J Pediatr Urol. 2015 Apr;11(2):67.e1-6. doi: 10.1016/j.jpurol.2014.09.010. Epub 2015 Feb 20. J Pediatr Urol. 2015. PMID: 25869826
-
Urethroplasty for urethral injuries and trauma-related strictures in children and adolescents: a single-institution experience.J Pediatr Urol. 2019 Apr;15(2):176.e1-176.e7. doi: 10.1016/j.jpurol.2018.11.014. Epub 2018 Nov 29. J Pediatr Urol. 2019. PMID: 30581060
-
Post-traumatic posterior urethral stricture in children: how to achieve a successful repair.J Pediatr Urol. 2008 Aug;4(4):290-4. doi: 10.1016/j.jpurol.2008.01.209. Epub 2008 Mar 10. J Pediatr Urol. 2008. PMID: 18644532
-
Complicated urethroplasty: a guide for surgeons.Nat Rev Urol. 2010 Sep;7(9):521-8. doi: 10.1038/nrurol.2010.118. Epub 2010 Aug 10. Nat Rev Urol. 2010. PMID: 20697432 Review.
-
[Management of male posterior urethral stenosis following trauma and prostatic treatments, techniques and results].Fr J Urol. 2024 Nov;34(11):102716. doi: 10.1016/j.fjurol.2024.102716. Fr J Urol. 2024. PMID: 39586656 Review. French.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
