

Long-Term Maternal and Child Outcomes Following Postnatal SSRI Treatment
- PMID: 37642961
- PMCID: PMC10466165
- DOI: 10.1001/jamanetworkopen.2023.31270
Long-Term Maternal and Child Outcomes Following Postnatal SSRI Treatment
Abstract
Importance: Although selective serotonin reuptake inhibitors (SSRIs) are recommended for postnatal depression treatment, there is a lack of evidence regarding long-term maternal and child outcomes following postnatal SSRI treatment.
Objective: To examine whether postnatal SSRI treatment moderated postnatal depression-associated maternal and child outcomes across early childhood years.
Design, setting, and participants: This cohort study used longitudinal data from the Norwegian Mother, Father and Child Cohort Study. Participating women were recruited in weeks 17 to 18 of pregnancy from 1999 to 2008 and were prospectively followed up after childbirth. Data analysis was performed between December 2021 to October 2022.
Exposure: Postnatal depression diagnosis (a binary indicator of eligibility for treatment) was defined as a score of 7 or greater on the 6-item version of the Edinburgh Postnatal Depression Scale. The Hopkins Symptom Checklist was used as a continuous indicator of and postnatal depressive symptomology at postpartum month 6. Postnatal SSRI treatment was identified using self-reported data at postpartum month 6.
Main outcomes and measures: Maternal outcomes included self-reported depression symptomology and relationship satisfaction from childbirth to postpartum year 5. Child outcomes included maternal-report internalizing and externalizing problems, attention-deficit/hyperactivity disorder symptoms, and motor and language development at ages 1.5, 3, and 5 years. A propensity score adjustment method was used to control for prenatal factors associated with postnatal SSRI exposure probability.
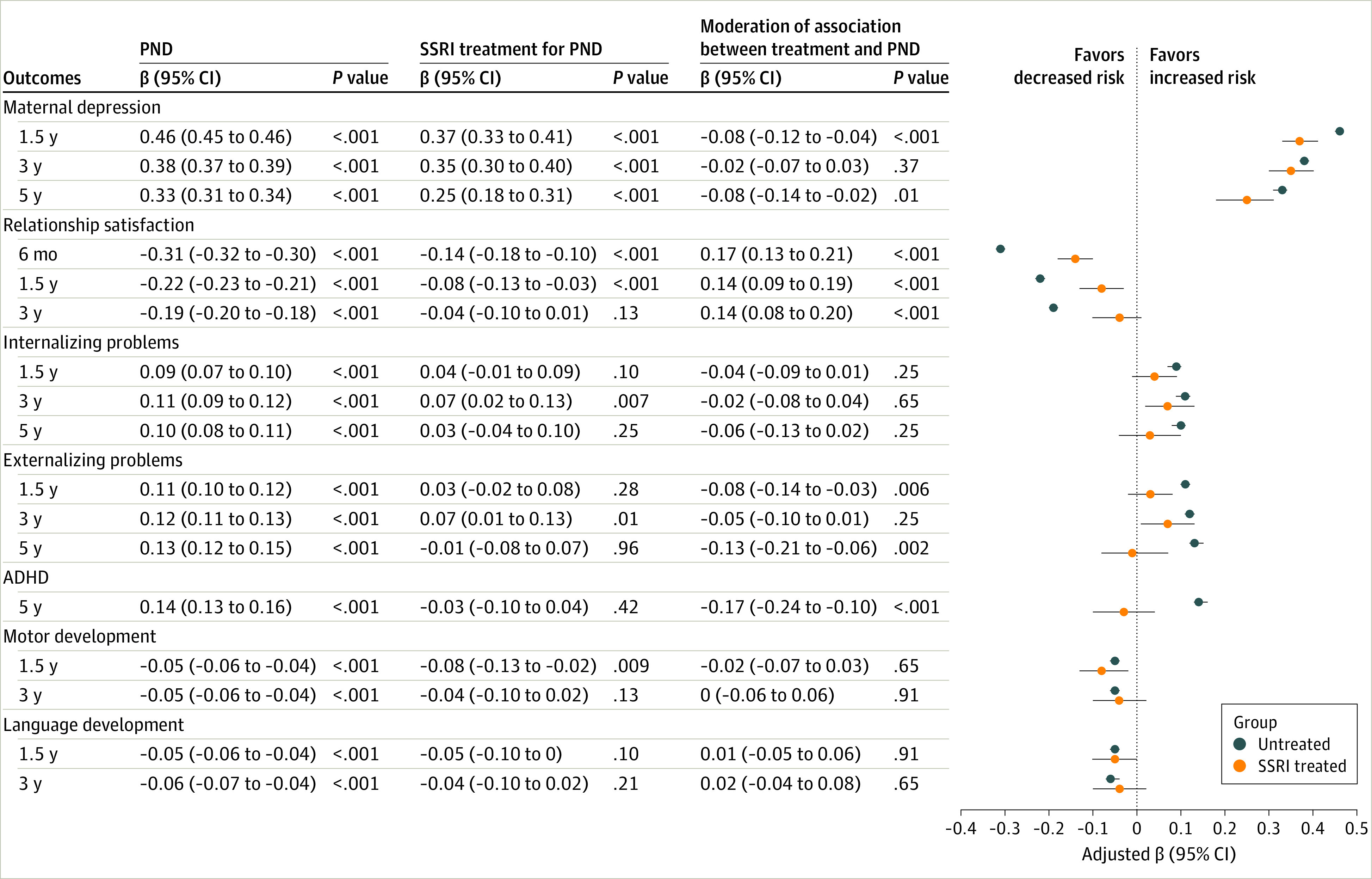
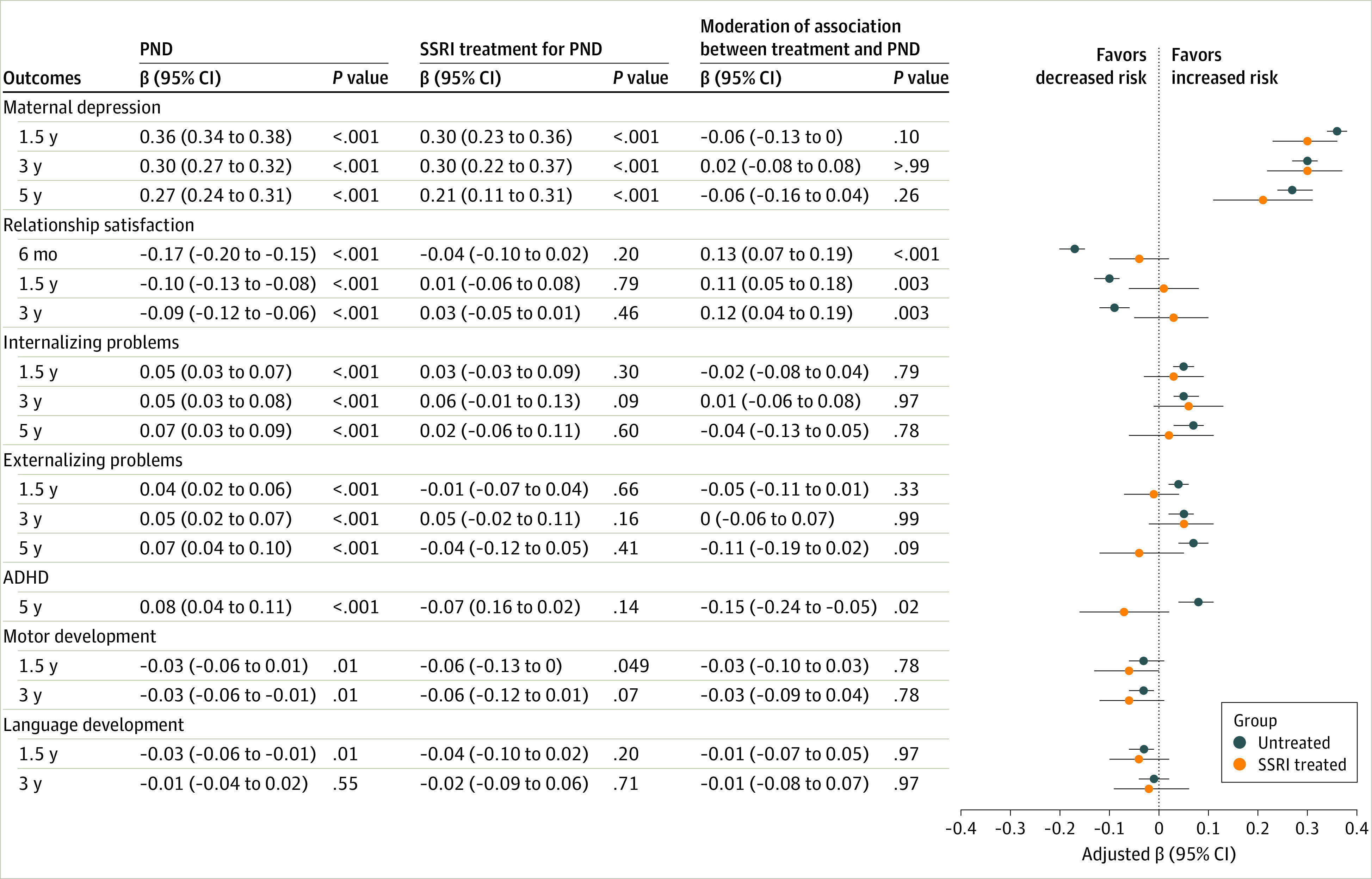
Results: Among a total of 61 081 mother-child dyads, 8671 (14.2%) (mean [SD] age, 29.93 [4.76] years) met the criteria for postnatal depression diagnosis, 177 (2.0%) (mean [SD] age, 30.20 [5.01] years) of whom received postnatal SSRI treatment. More severe postnatal depression symptomology was associated with a range of adverse maternal and child outcomes. Focusing analyses only on the postnatal depression dyads indicated that postnatal SSRI treatment attenuated negative associations between postnatal depression and maternal relationship satisfaction at postpartum month 6 (moderation β, 0.13; 95% CI, 0.07-0.19), years 1.5 (moderation β, 0.11; 95% CI, 0.05-0.18) and 3 (moderation β, 0.12; 95% CI, 0.04-0.19), and for child ADHD at age 5 years (moderation β, -0.15; 95% CI, -0.24 to -0.05). Postnatal SSRI treatment mitigated the negative associations between postnatal depression and maternal depression, partner relationship satisfaction, child externalizing problems, and attention-deficit/hyperactivity disorder up to 5 years after childbirth.
Conclusions and relevance: The results of this large prospective cohort study suggest that postnatal SSRI treatment was associated with a reduced risk of postnatal depression-associated maternal mental health problems and child externalizing behaviors across early childhood years. These findings suggest that postnatal SSRI treatment may bring benefits in the long term to women with postnatal depression and their offspring. This study potentially provides valuable information for clinicians and women with postnatal depression to make informed treatment decisions.
Conflict of interest statement
Figures
Similar articles
-
Analysis of Maternal Postnatal Depression, Socioeconomic Factors, and Offspring Internalizing Symptoms in a Longitudinal Cohort in South Africa.JAMA Netw Open. 2021 Aug 2;4(8):e2121667. doi: 10.1001/jamanetworkopen.2021.21667. JAMA Netw Open. 2021. PMID: 34410394 Free PMC article.
-
Trajectories of maternal depressive symptoms during pregnancy and the first 12 months postpartum and child externalizing and internalizing behavior at three years.PLoS One. 2018 Apr 13;13(4):e0195365. doi: 10.1371/journal.pone.0195365. eCollection 2018. PLoS One. 2018. PMID: 29652937 Free PMC article.
-
Prenatal effects of selective serotonin reuptake inhibitor antidepressants, serotonin transporter promoter genotype (SLC6A4), and maternal mood on child behavior at 3 years of age.Arch Pediatr Adolesc Med. 2010 May;164(5):444-51. doi: 10.1001/archpediatrics.2010.51. Arch Pediatr Adolesc Med. 2010. PMID: 20439795
-
Antidepressant Treatment of Depression During Pregnancy and the Postpartum Period.Evid Rep Technol Assess (Full Rep). 2014 Jul;(216):1-308. doi: 10.23970/AHRQEPCERTA216. Evid Rep Technol Assess (Full Rep). 2014. PMID: 30313002 Review.
-
Socioeconomic factors and sex effects of postpartum maternal depression on offspring internalizing symptoms: a systematic review and meta-analysis.BMC Med. 2025 Feb 6;23(1):69. doi: 10.1186/s12916-025-03877-7. BMC Med. 2025. PMID: 39915783 Free PMC article.
Cited by
-
[Risk of postpartum depression in primary care].Rev Med Inst Mex Seguro Soc. 2024 Jul 1;62(4):1-7. doi: 10.5281/zenodo.11397005. Rev Med Inst Mex Seguro Soc. 2024. PMID: 39541250 Free PMC article. Spanish.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
