

Investigating the role of platelets and platelet-derived transforming growth factor-β in idiopathic pulmonary fibrosis
- PMID: 37643008
- PMCID: PMC10639018
- DOI: 10.1152/ajplung.00227.2022
Investigating the role of platelets and platelet-derived transforming growth factor-β in idiopathic pulmonary fibrosis
Abstract
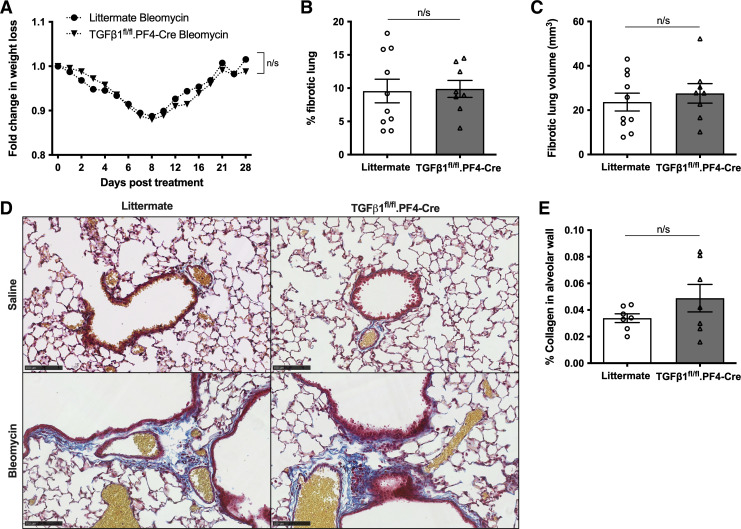
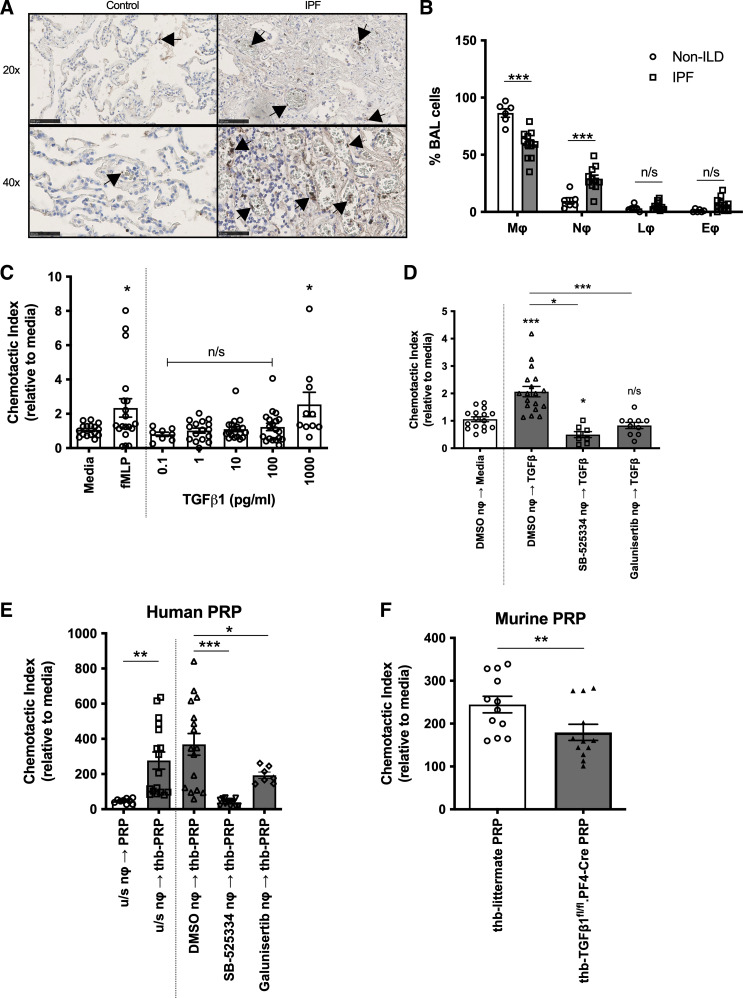
Transforming growth factor-β1 (TGFβ1) is the key profibrotic cytokine in idiopathic pulmonary fibrosis (IPF), but the primary source of this cytokine in this disease is unknown. Platelets have abundant stores of TGFβ1, although the role of these cells in IPF is ill-defined. In this study, we investigated whether platelets, and specifically platelet-derived TGFβ1, mediate IPF disease progression. Patients with IPF and non-IPF patients were recruited to determine platelet reactivity, and separate cohorts of patients with IPF were followed for mortality. To study whether platelet-derived TGFβ1 modulates pulmonary fibrosis (PF), mice with a targeted deletion of TGFβ1 in megakaryocytes and platelets (TGFβ1fl/fl.PF4-Cre) were used in the well-characterized bleomycin-induced pulmonary fibrosis (PF) animal model. In a discovery cohort, we found significantly higher mortality in patients with IPF who had elevated platelet counts within the normal range. However, our validation cohort did not confirm this observation, despite significantly increased platelets, neutrophils, active TGFβ1, and CCL5, a chemokine produced by inflammatory cells, in the blood, lung, and bronchoalveolar lavage (BAL) of patients with IPF. In vivo, we showed that despite platelets being readily detected within the lungs of bleomycin-treated mice, neither the degree of pulmonary inflammation nor fibrosis was significantly different between TGFβ1fl/fl.PF4-Cre and control mice. Our results demonstrate for the first time that platelet-derived TGFβ1 does not significantly mediate inflammation or fibrosis in a PF animal model. Furthermore, our human studies revealed blood platelet counts do not consistently predict mortality in IPF but other platelet-derived mediators, such as C-C chemokine ligand 5 (CCL5), may promote neutrophil recruitment and human IPF.NEW & NOTEWORTHY Platelets are a rich source of profibrotic TGFβ; however, the role of platelets in idiopathic pulmonary fibrosis (IPF) is unclear. We identified that patients with IPF have significantly more platelets, neutrophils, and active TGFβ in their airways than control patients. Using an animal model of IPF, we demonstrated that platelet-derived TGFβ does not significantly drive lung fibrosis or inflammation. Our findings offer a better understanding of platelets in both human and animal studies of IPF.
Keywords: inflammation; interstitial lung diseases; platelets; pulmonary fibrosis; transforming growth factor-β1.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures





References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous