

Atezolizumab Combined With Bevacizumab and Platinum-Based Therapy for Platinum-Sensitive Ovarian Cancer: Placebo-Controlled Randomized Phase III ATALANTE/ENGOT-ov29 Trial
- PMID: 37643382
- PMCID: PMC10602539
- DOI: 10.1200/JCO.23.00529
Atezolizumab Combined With Bevacizumab and Platinum-Based Therapy for Platinum-Sensitive Ovarian Cancer: Placebo-Controlled Randomized Phase III ATALANTE/ENGOT-ov29 Trial
Abstract
Purpose: Platinum-based doublets with concurrent and maintenance bevacizumab are standard therapy for ovarian cancer (OC) relapsing after a platinum-free interval (PFI) >6 months. Immunotherapy may be synergistic with bevacizumab and chemotherapy.
Patients and methods: ATALANTE/ENGOT-ov29 (ClinicalTrials.gov identifier: NCT02891824), a placebo-controlled double-blinded randomized phase III trial, enrolled patients with recurrent epithelial OC, one to two previous chemotherapy lines, and PFI >6 months. Eligible patients were randomly assigned 2:1 to atezolizumab (1,200 mg once every 3 weeks or equivalent) or placebo for up to 24 months, combined with bevacizumab and six cycles of chemotherapy doublet, stratified by PFI, PD-L1 status, and chemotherapy regimen. Coprimary end points were investigator-assessed progression-free survival (PFS) in the intention-to-treat (ITT) and PD-L1-positive populations (alpha .025 for each population).
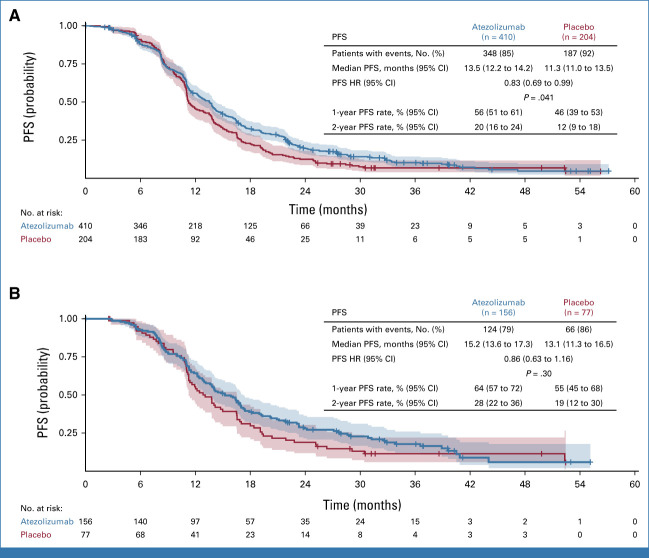
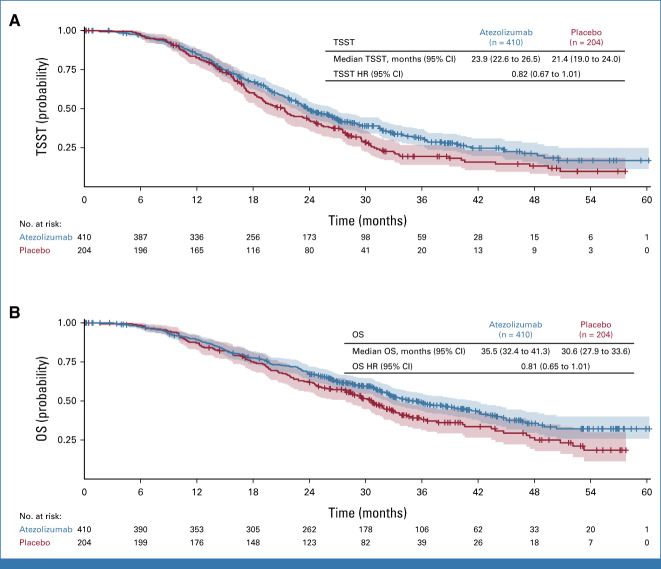
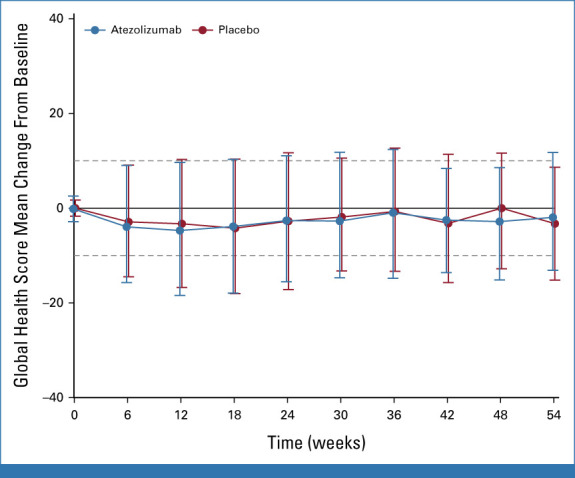
Results: Between September 2016 and October 2019, 614 patients were randomly assigned: 410 to atezolizumab and 204 to placebo. Only 38% had PD-L1-positive tumors. After 3 years' median follow-up, the PFS difference between atezolizumab and placebo did not reach statistical significance in the ITT (hazard ratio [HR], 0.83; 95% CI, 0.69 to 0.99; P = .041; median 13.5 v 11.3 months, respectively) or PD-L1-positive (HR, 0.86; 95% CI, 0.63 to 1.16; P = .30; median 15.2 v 13.1 months, respectively) populations. The immature overall survival (OS) HR was 0.81 (95% CI, 0.65 to 1.01; median 35.5 v 30.6 months with atezolizumab v placebo, respectively). Global health-related quality of life did not differ between treatment arms. Grade ≥3 adverse events (AEs) occurred in 88% of atezolizumab-treated and 87% of placebo-treated patients; grade ≥3 AEs typical of immunotherapy were more common with atezolizumab (13% v 8%, respectively).
Conclusion: ATALANTE/ENGOT-ov29 did not meet its coprimary PFS objectives in the ITT or PD-L1-positive populations. OS follow-up continues. Further research on biopsy samples is warranted to decipher the immunologic landscape of late-relapsing OC.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures

References
-
- Tewari KS, Monk BJ, Vergote I, et al. : Survival with cemiplimab in recurrent cervical cancer. N Engl J Med 386:544-555, 2022 - PubMed
-
- Colombo N, Dubot C, Lorusso D, et al. : Pembrolizumab for persistent, recurrent, or metastatic cervical cancer. N Engl J Med 385:1856-1867, 2021 - PubMed
-
- Socinski MA, Jotte RM, Cappuzzo F, et al. : Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N Engl J Med 378:2288-2301, 2018 - PubMed
-
- Rini BI, Plimack ER, Stus V, et al. : Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med 380:1116-1127, 2019 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
