

Identification of distinct clinical phenotypes of cardiogenic shock using machine learning consensus clustering approach
- PMID: 37644414
- PMCID: PMC10466857
- DOI: 10.1186/s12872-023-03380-y
Identification of distinct clinical phenotypes of cardiogenic shock using machine learning consensus clustering approach
Abstract
Background: Cardiogenic shock (CS) is a complex state with many underlying causes and associated outcomes. It is still difficult to differentiate between various CS phenotypes. We investigated if the CS phenotypes with distinctive clinical profiles and prognoses might be found using the machine learning (ML) consensus clustering approach.
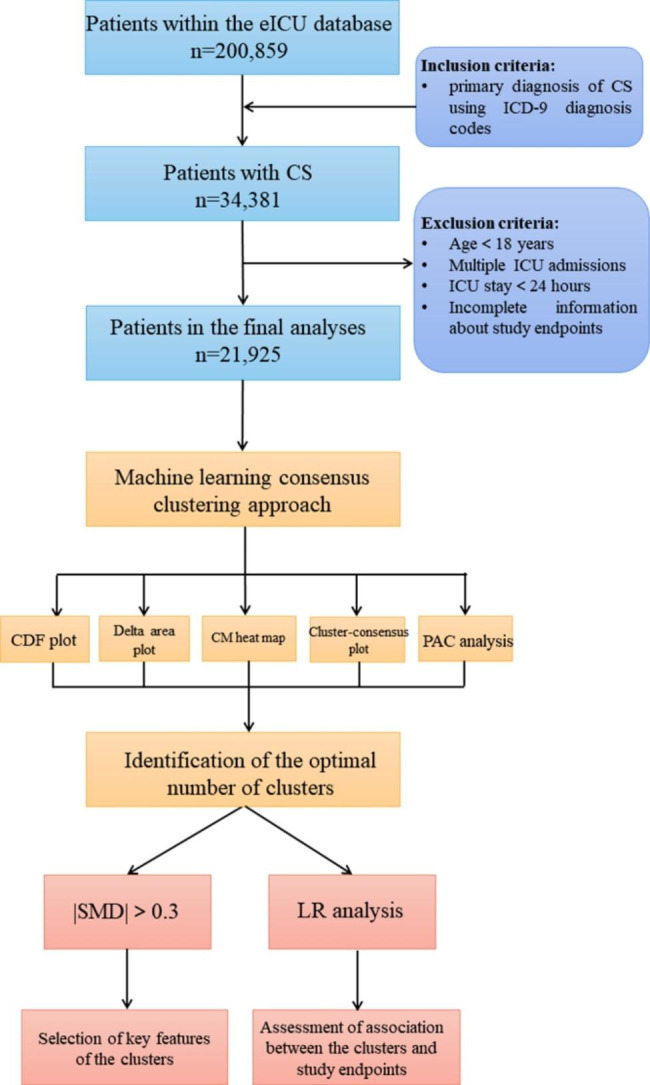
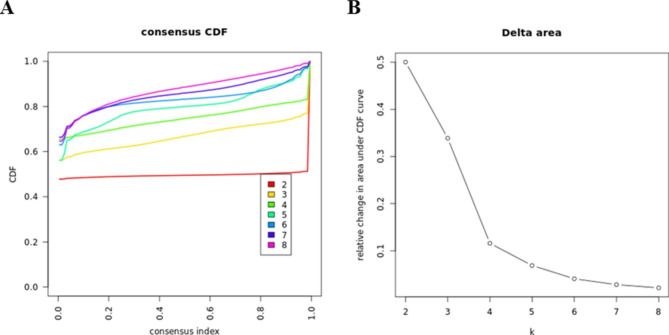
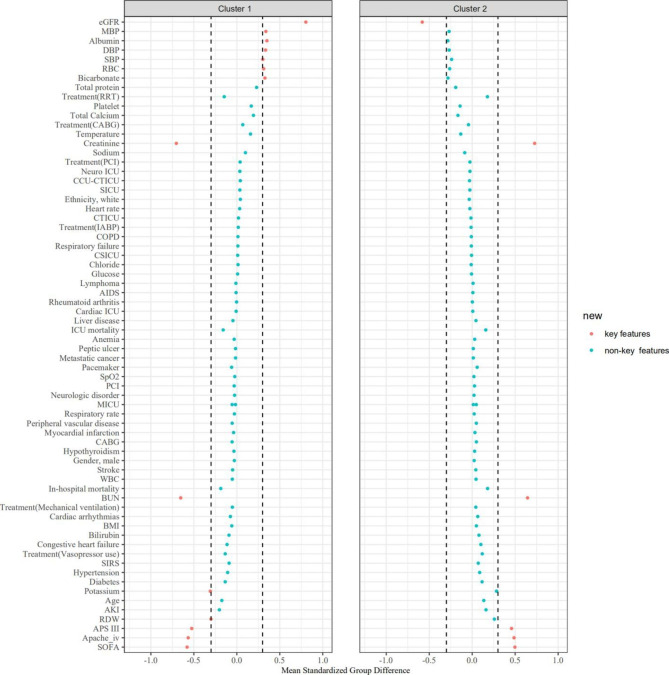
Methods: The current study included patients who were diagnosed with CS at the time of admission from the electronic ICU (eICU) Collaborative Research Database. Among 21,925 patients with CS, an unsupervised ML consensus clustering analysis was conducted. The optimal number of clusters was identified by means of the consensus matrix (CM) heat map, cumulative distribution function (CDF), cluster-consensus plots, and the proportion of ambiguously clustered pairs (PAC) analysis. We calculated the standardized mean difference (SMD) of each variable and used the cutoff of ± 0.3 to identify each cluster's key features. We examined the relationship between the phenotypes and several clinical endpoints utilizing logistic regression (LR) analysis.
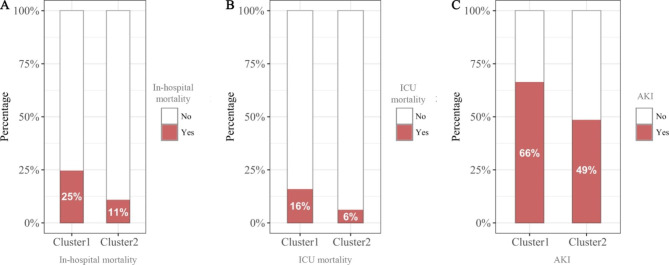
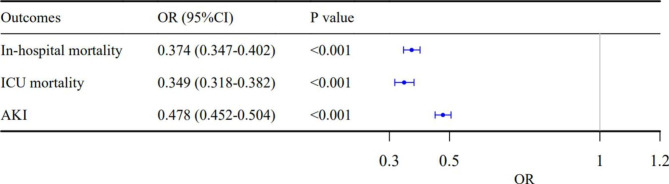
Results: The consensus cluster analysis identified two clusters (Cluster 1: n = 9,848; Cluster 2: n = 12,077). The key features of patients in Cluster 1, compared with Cluster 2, included: lower blood pressure, lower eGFR (estimated glomerular filtration rate), higher BUN (blood urea nitrogen), higher creatinine, lower albumin, higher potassium, lower bicarbonate, lower red blood cell (RBC), higher red blood cell distribution width (RDW), higher SOFA score, higher APS III score, and higher APACHE IV score on admission. The results of LR analysis showed that the Cluster 2 was associated with lower in-hospital mortality (odds ratio [OR]: 0.374; 95% confidence interval [CI]: 0.347-0.402; P < 0.001), ICU mortality (OR: 0.349; 95% CI: 0.318-0.382; P < 0.001), and the incidence of acute kidney injury (AKI) after admission (OR: 0.478; 95% CI: 0.452-0.505; P < 0.001).
Conclusions: ML consensus clustering analysis synthesized the pattern of clinical and laboratory data to reveal distinct CS phenotypes with different clinical outcomes.
Keywords: Acute kidney injury; Artificial intelligence; Cardiogenic shock; Cluster; Intensive care unit; Machine learning; Mortality; Phenotype.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Distinct phenotypes of hospitalized patients with hyperkalemia by machine learning consensus clustering and associated mortality risks.QJM. 2022 Jul 9;115(7):442-449. doi: 10.1093/qjmed/hcab194. QJM. 2022. PMID: 34270780
-
Clinically Distinct Subtypes of Acute Kidney Injury on Hospital Admission Identified by Machine Learning Consensus Clustering.Med Sci (Basel). 2021 Sep 24;9(4):60. doi: 10.3390/medsci9040060. Med Sci (Basel). 2021. PMID: 34698185 Free PMC article.
-
Validation of cardiogenic shock phenotypes in a mixed cardiac intensive care unit population.Catheter Cardiovasc Interv. 2022 Mar;99(4):1006-1014. doi: 10.1002/ccd.30103. Epub 2022 Jan 25. Catheter Cardiovasc Interv. 2022. PMID: 35077592
-
Cardiogenic shock and machine learning: A systematic review on prediction through clinical decision support softwares.J Card Surg. 2021 Nov;36(11):4153-4159. doi: 10.1111/jocs.15934. Epub 2021 Aug 31. J Card Surg. 2021. PMID: 34463361
-
Machine Learning Approaches for Phenotyping in Cardiogenic Shock and Critical Illness: Part 2 of 2.JACC Adv. 2022 Oct 28;1(4):100126. doi: 10.1016/j.jacadv.2022.100126. eCollection 2022 Oct. JACC Adv. 2022. PMID: 38939698 Free PMC article. Review.
Cited by
-
Temporary Mechanical Support in Cardiogenic Shock Secondary to Heart Failure: An Evolving Paradigm.J Pers Med. 2025 May 2;15(5):184. doi: 10.3390/jpm15050184. J Pers Med. 2025. PMID: 40423056 Free PMC article. Review.
-
The Heart of Transformation: Exploring Artificial Intelligence in Cardiovascular Disease.Biomedicines. 2025 Feb 10;13(2):427. doi: 10.3390/biomedicines13020427. Biomedicines. 2025. PMID: 40002840 Free PMC article. Review.
-
Profiling of Cardiogenic Shock: Incorporating Machine Learning Into Bedside Management.J Soc Cardiovasc Angiogr Interv. 2024 May 28;4(3Part B):102047. doi: 10.1016/j.jscai.2024.102047. eCollection 2025 Mar. J Soc Cardiovasc Angiogr Interv. 2024. PMID: 40230675 Free PMC article. Review.
-
Revolutionizing Cardiology through Artificial Intelligence-Big Data from Proactive Prevention to Precise Diagnostics and Cutting-Edge Treatment-A Comprehensive Review of the Past 5 Years.Diagnostics (Basel). 2024 May 26;14(11):1103. doi: 10.3390/diagnostics14111103. Diagnostics (Basel). 2024. PMID: 38893630 Free PMC article. Review.
-
Machine learning consensus clustering for inflammatory subtype analysis in stroke and its impact on mortality risk: a study based on NHANES (1999-2018).Front Neurol. 2025 Apr 10;16:1562247. doi: 10.3389/fneur.2025.1562247. eCollection 2025. Front Neurol. 2025. PMID: 40276469 Free PMC article.
References
-
- van Diepen S, Katz JN, Albert NM, Henry TD, Jacobs AK, Kapur NK, Kilic A, Menon V, Ohman EM, Sweitzer NK, et al. Contemporary Management of cardiogenic shock: a Scientific Statement from the American Heart Association. Circulation. 2017;136(16):e232–68. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
