

Outpatient visits before and after Lyme disease diagnosis in a Maryland employer-based health plan
- PMID: 37644525
- PMCID: PMC10466890
- DOI: 10.1186/s12913-023-09909-3
Outpatient visits before and after Lyme disease diagnosis in a Maryland employer-based health plan
Abstract
Background: Insurance claims data have been used to inform an understanding of Lyme disease epidemiology and cost of care, however few such studies have incorporated post-treatment symptoms following diagnosis. Using longitudinal data from a private, employer-based health plan in an endemic US state, we compared outpatient care utilization pre- and post-Lyme disease diagnosis. We hypothesized that utilization would be higher in the post-diagnosis period, and that temporal trends would differ by age and gender.
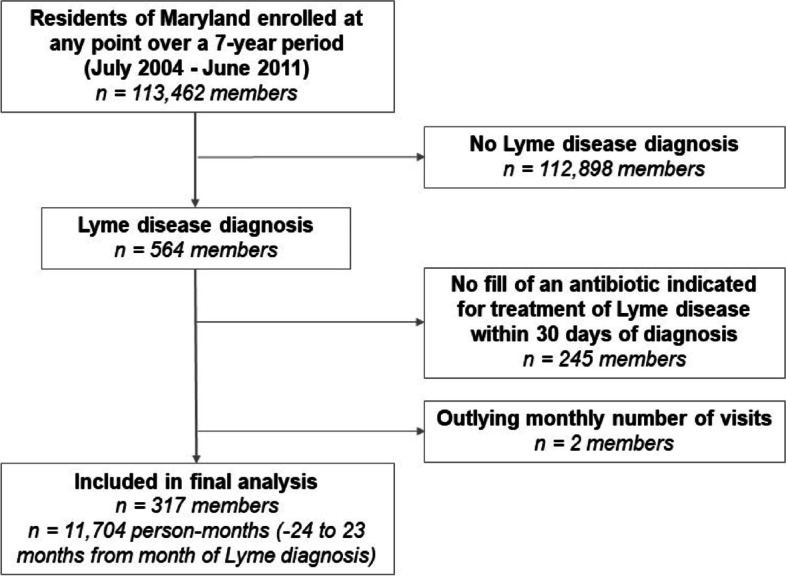
Methods: Members with Lyme disease were required to have both a corresponding ICD-9 code and a fill of an antibiotic indicated for treatment of the infection within 30 days of diagnosis. A 2-year 'pre- diagnosis' period and a 2-year 'post-diagnosis period' were centered around the diagnosis month. Lyme disease-relevant outpatient care visits were defined as specific primary care, specialty care, or urgent care visits. Descriptive statistics examined visits during these pre- and post-diagnosis periods, and the association between these periods and the number of visits was explored using generalized linear mixed effects models adjusting for age, season of the year, and gender.
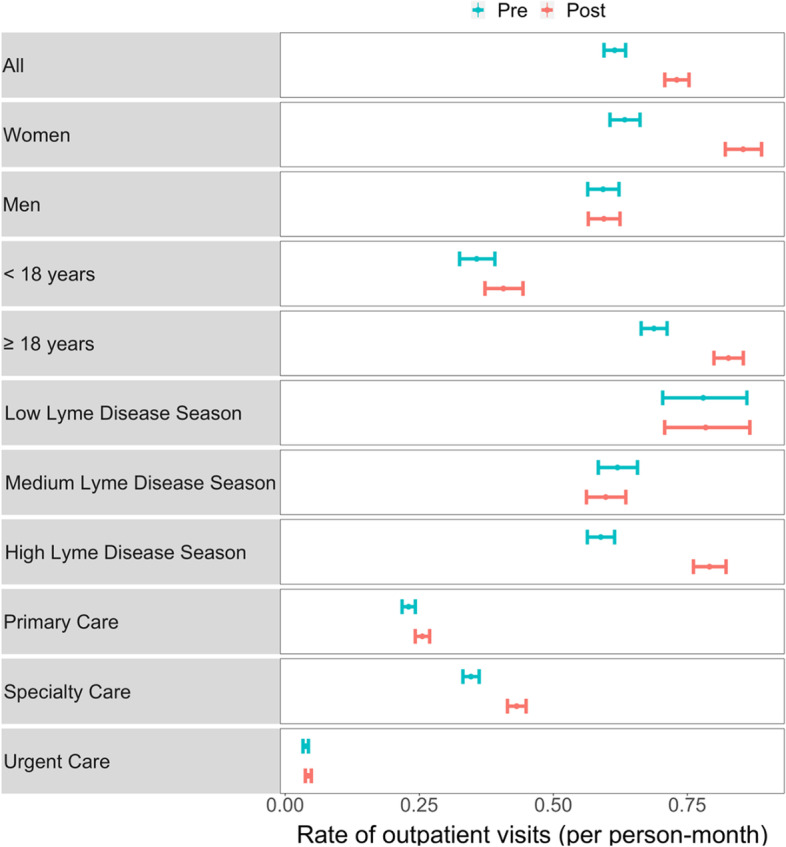
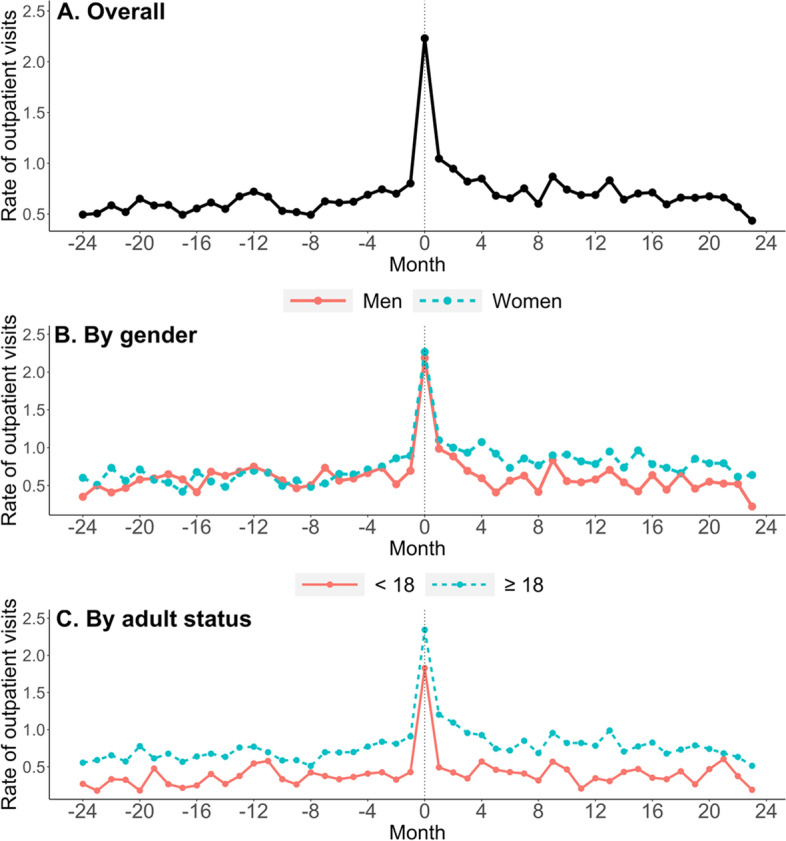
Results: The rate of outpatient visits increased 26% from the pre to the post-Lyme disease diagnosis periods among our 317-member sample (rate ratio = 1.26 [1.18, 1.36], p < 0.001). Descriptively, care utilization increases appeared to persist across months in the post-diagnosis period. Women's care utilization increased by 36% (1.36 [1.24, 1.50], p < 0.001), a significantly higher increase than the 14% increase found among men (1.14 [1.02, 1.27], p = 0.017). This gender difference was mainly driven by adult members. We found a borderline significant 17% increase in visits for children < 18 years, (1.17 [0.99, 1.38], p = 0.068), and a 31% increase for adults ≥ 18 years (1.31 [1.21, 1.42], p < 0.001).
Conclusions: Although modest at the population level, the statistically significant increases in post-Lyme diagnosis outpatient care we observed were persistent and unevenly distributed across demographic and place of service categories. As Lyme disease cases continue to grow, so will the cumulative prevalence of persistent symptoms after treatment. Therefore, it will be important to confirm these findings and understand their significance for care utilization and cost, particularly against the backdrop of other post-acute infectious syndromes.
Keywords: Claims analysis; Lyme disease; Maryland; Post-treatment Lyme disease; Tick-borne diseases.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
JNA received consulting fees from the Pfizer North America Lyme Disease Vaccine Ad Board, has provided expert testimony in malpractice cases, and has been issued the following patent: Elevated CCL19 after completion of therapy for acute Lyme disease identifies patients at risk for development of post-treatment Lyme disease who will benefit from further antibiotic therapy. The remaining authors declare that they have no competing interests.
Figures
Similar articles
-
Health care costs, utilization and patterns of care following Lyme disease.PLoS One. 2015 Feb 4;10(2):e0116767. doi: 10.1371/journal.pone.0116767. eCollection 2015. PLoS One. 2015. PMID: 25650808 Free PMC article.
-
Incidence of Lyme Disease Diagnosis in a Maryland Medicaid Population, 2004-2011.Am J Epidemiol. 2018 Oct 1;187(10):2202-2209. doi: 10.1093/aje/kwy133. Am J Epidemiol. 2018. PMID: 29955850
-
Classification of patients referred under suspicion of tick-borne diseases, Copenhagen, Denmark.Ticks Tick Borne Dis. 2021 Jan;12(1):101591. doi: 10.1016/j.ttbdis.2020.101591. Epub 2020 Oct 9. Ticks Tick Borne Dis. 2021. PMID: 33126203
-
Emergency department presentations of Lyme disease in children.Pediatr Emerg Care. 1998 Oct;14(5):356-61. Pediatr Emerg Care. 1998. PMID: 9814407 Review.
-
The prevalence and burden of migraine and severe headache in the United States: updated statistics from government health surveillance studies.Headache. 2015 Jan;55(1):21-34. doi: 10.1111/head.12482. Headache. 2015. PMID: 25600719 Review.
Cited by
-
Optimizing identification of Lyme disease diagnoses in commercial insurance claims data, United States, 2016-2019.BMC Infect Dis. 2024 Nov 20;24(1):1322. doi: 10.1186/s12879-024-10195-5. BMC Infect Dis. 2024. PMID: 39567874 Free PMC article.
-
Estimating the incidence of autoimmune inflammatory arthritis after Lyme disease.Semin Arthritis Rheum. 2025 Jul 16;74:152797. doi: 10.1016/j.semarthrit.2025.152797. Online ahead of print. Semin Arthritis Rheum. 2025. PMID: 40706260
References
-
- Centers for Disease Control and Prevention. Lyme Disease Data and Surveillance. Available from: https://www.cdc.gov/lyme/datasurveillance/index.html. [Cited 2022 Sep 26].
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
