Expanding the spectrum of neonatal-onset AIFM1-associated disorders
- PMID: 37644805
- PMCID: PMC10578896
- DOI: 10.1002/acn3.51876
Expanding the spectrum of neonatal-onset AIFM1-associated disorders
Abstract
Objectives: Pathogenic variants in AIFM1 have been associated with a wide spectrum of disorders, spanning from CMT4X to mitochondrial encephalopathy. Here we present a novel phenotype and review the existing literature on AIFM1-related disorders.
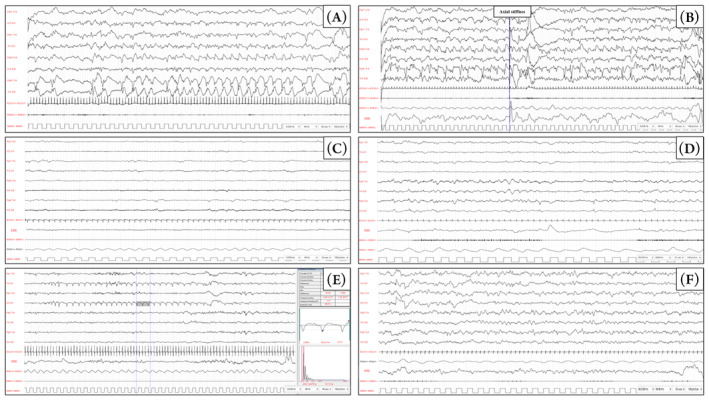
Methods: We performed EEG recordings, brain MRI and MR Spectroscopy, metabolic screening, echocardiogram, clinical exome sequencing (CES) and family study. Effects of the variant were established on cultured fibroblasts from skin punch biopsy.
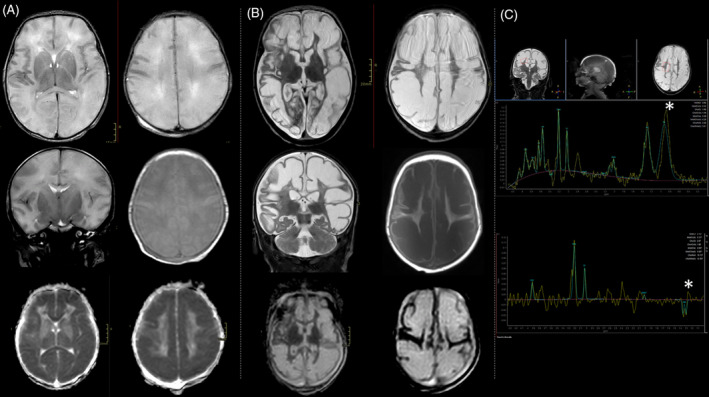
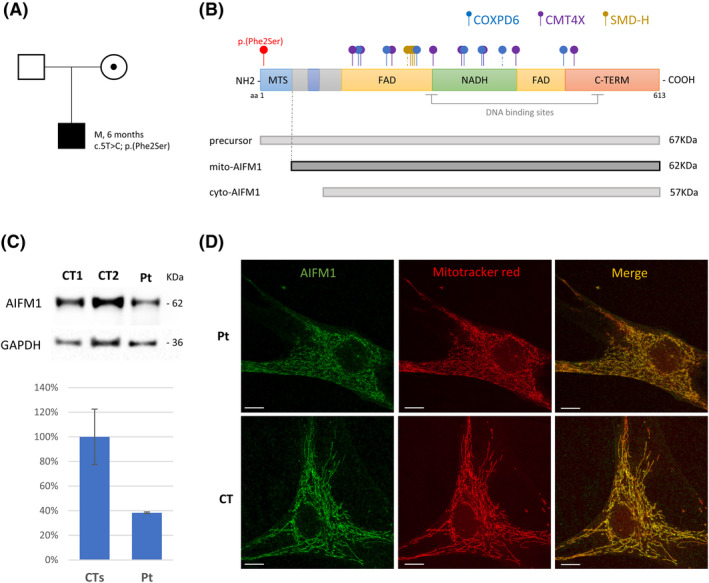
Results: The patient presented with drug-resistant, electro-clinical, multifocal seizures 6 h after birth. Brain MRI revealed prominent brain swelling of both hemispheres and widespread signal alteration in large part of the cortex and of the thalami, with sparing of the basal nuclei. CES analysis revealed the likely pathogenic variant c.5T>C; p.(Phe2Ser) in the AIFM1 gene. The affected amino acid residue is located in the mitochondrial targeting sequence. Functional studies on cultured fibroblast showed a clear reduction in AIFM1 protein amount and defective activities of respiratory chain complexes I, III and IV. No evidence of protein mislocalization or accumulation of precursor protein was observed. Riboflavin, Coenzyme Q10 and thiamine supplementation was therefore given. At 6 months of age, the patient exhibited microcephaly but did not experience any further deterioration. He is still fed orally and there is no evidence of muscle weakness or atrophy.
Interpretation: This is the first AIFM1 case associated with neonatal seizures and diffuse white matter involvement with relative sparing of basal ganglia, in the absence of clinical signs suggestive of myopathy or motor neuron disease.
© 2023 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
The authors have no disclosures to report regarding the present study.
Figures