

Facilitators and Barriers to Interacting With Clinical Decision Support in the ICU: A Mixed-Methods Approach
- PMID: 37644969
- PMCID: PMC10461946
- DOI: 10.1097/CCE.0000000000000967
Facilitators and Barriers to Interacting With Clinical Decision Support in the ICU: A Mixed-Methods Approach
Abstract
Objectives: Clinical decision support systems (CDSSs) are used in various aspects of healthcare to improve clinical decision-making, including in the ICU. However, there is growing evidence that CDSS are not used to their full potential, often resulting in alert fatigue which has been associated with patient harm. Clinicians in the ICU may be more vulnerable to desensitization of alerts than clinicians in less urgent parts of the hospital. We evaluated facilitators and barriers to appropriate CDSS interaction and provide methods to improve currently available CDSS in the ICU.
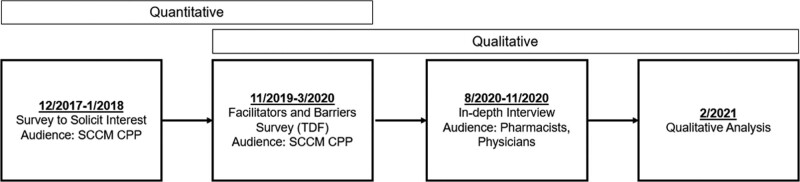
Design: Sequential explanatory mixed-methods study design, using the BEhavior and Acceptance fRamework.
Setting: International survey study.
Patient/subjects: Clinicians (pharmacists, physicians) identified via survey, with recent experience with clinical decision support.
Interventions: An initial survey was developed to evaluate clinician perspectives on their interactions with CDSS. A subsequent in-depth interview was developed to further evaluate clinician (pharmacist, physician) beliefs and behaviors about CDSS. These interviews were then qualitatively analyzed to determine themes of facilitators and barriers with CDSS interactions.
Measurements and main results: A total of 48 respondents completed the initial survey (estimated response rate 15.5%). The majority believed that responding to CDSS alerts was part of their job (75%) but felt they experienced alert fatigue (56.5%). In the qualitative analysis, a total of five facilitators (patient safety, ease of response, specificity, prioritization, and feedback) and four barriers (excess quantity, work environment, difficulty in response, and irrelevance) were identified from the in-depth interviews.
Conclusions: In this mixed-methods survey, we identified areas that institutions should focus on to improve appropriate clinician interactions with CDSS, specific to the ICU. Tailoring of CDSS to the ICU may lead to improvement in CDSS and subsequent improved patient safety outcomes.
Keywords: alert fatigue; clinical decision support systems; implementation science; intensive care unit; patient safety.
Copyright © 2023 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Bates reports grants and personal fees from EarlySense, personal fees from Center for Digital Innovation Negev, equity from ValeraHealth, equity from Clew, equity from MDClone, personal fees and equity from AESOP, personal fees and equity from Feelbetter, equity from Guided Clinical Solutions, and grants from International Business Machines Corporation Watson Health, outside the submitted work. Dr. Bates has a patent pending (PHC-028564 US Patent Cooperation Treaty), on intraoperative clinical decision support. Dr. Kane-Gill receives grant funding from the National Institute of Diabetes and Digestive and Kidney Diseases R01DK121730 and U01DK130010, the National Center for Complementary and Integrative Health U54AT008909, and the Jewish Healthcare Foundation. Drs. Sorce and Kane-Gill also hold executive positions in the Society of Critical Care Medicine. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Similar articles
-
Acceptance, Barriers, and Facilitators to Implementing Artificial Intelligence-Based Decision Support Systems in Emergency Departments: Quantitative and Qualitative Evaluation.JMIR Form Res. 2022 Jun 13;6(6):e36501. doi: 10.2196/36501. JMIR Form Res. 2022. PMID: 35699995 Free PMC article.
-
Barriers and facilitators to the adoption of electronic clinical decision support systems: a qualitative interview study with UK general practitioners.BMC Med Inform Decis Mak. 2021 Jun 21;21(1):193. doi: 10.1186/s12911-021-01557-z. BMC Med Inform Decis Mak. 2021. PMID: 34154580 Free PMC article.
-
Tackling alert fatigue with a semi-automated clinical decision support system: quantitative evaluation and end-user survey.Swiss Med Wkly. 2023 Jul 7;153:40082. doi: 10.57187/smw.2023.40082. Swiss Med Wkly. 2023. PMID: 37454289
-
Evaluating the alert appropriateness of clinical decision support systems in supporting clinical workflow.J Biomed Inform. 2020 Jun;106:103453. doi: 10.1016/j.jbi.2020.103453. Epub 2020 May 14. J Biomed Inform. 2020. PMID: 32417444 Review.
-
Clinical Decision Support Systems for Drug Allergy Checking: Systematic Review.J Med Internet Res. 2018 Sep 7;20(9):e258. doi: 10.2196/jmir.8206. J Med Internet Res. 2018. PMID: 30194058 Free PMC article.
Cited by
-
Exploring intensive care unit nurses' acceptance of clinical decision support systems and use of volumetric pump data: A qualitative description study.Nurs Crit Care. 2025 Mar;30(2):e13274. doi: 10.1111/nicc.13274. Nurs Crit Care. 2025. PMID: 40012078 Free PMC article.
-
Impact of automated pop-up alerts on simultaneous prescriptions of antimicrobial agents and metal cations.J Pharm Health Care Sci. 2024 Sep 27;10(1):59. doi: 10.1186/s40780-024-00377-3. J Pharm Health Care Sci. 2024. PMID: 39334329 Free PMC article.
-
Machine Learning for Targeted Advance Care Planning in Cancer Patients: A Quality Improvement Study.J Pain Symptom Manage. 2024 Dec;68(6):539-547.e3. doi: 10.1016/j.jpainsymman.2024.08.036. Epub 2024 Sep 3. J Pain Symptom Manage. 2024. PMID: 39237028
References
-
- Oei SP, van Sloun RJG, van der Ven M, et al. : Towards early sepsis detection from measurements at the general ward through deep learning. Intell Based Med 2021; 5:100042
-
- Colpaert K, Hoste EA, Steurbaut K, et al. : Impact of real-time electronic alerting of acute kidney injury on therapeutic intervention and progression of RIFLE class. Crit Care Med 2012; 40:1164–1170 - PubMed
-
- Kane-Gill SL, O’Connor MF, Rothschild JM, et al. : Technologic distractions (Part 1): Summary of approaches to manage alert quantity with intent to reduce alert fatigue and suggestions for alert fatigue metrics. Crit Care Med 2017; 45:1481–1488 - PubMed
LinkOut - more resources
Full Text Sources
