

Delayed Treatment of Bloodstream Infection at Admission is Associated With Initial Low Early Warning Score and Increased Mortality
- PMID: 37644974
- PMCID: PMC10461960
- DOI: 10.1097/CCE.0000000000000959
Delayed Treatment of Bloodstream Infection at Admission is Associated With Initial Low Early Warning Score and Increased Mortality
Abstract
Objectives: To identify factors associated with antibiotic treatment delay in patients admitted with bloodstream infections (BSIs).
Design: Retrospective cohort study.
Setting: North Zealand Hospital, Denmark.
Patients: Adult patients with positive blood cultures obtained within the first 48 hours of admission between January 1, 2015, and December 31, 2015 (n = 926).
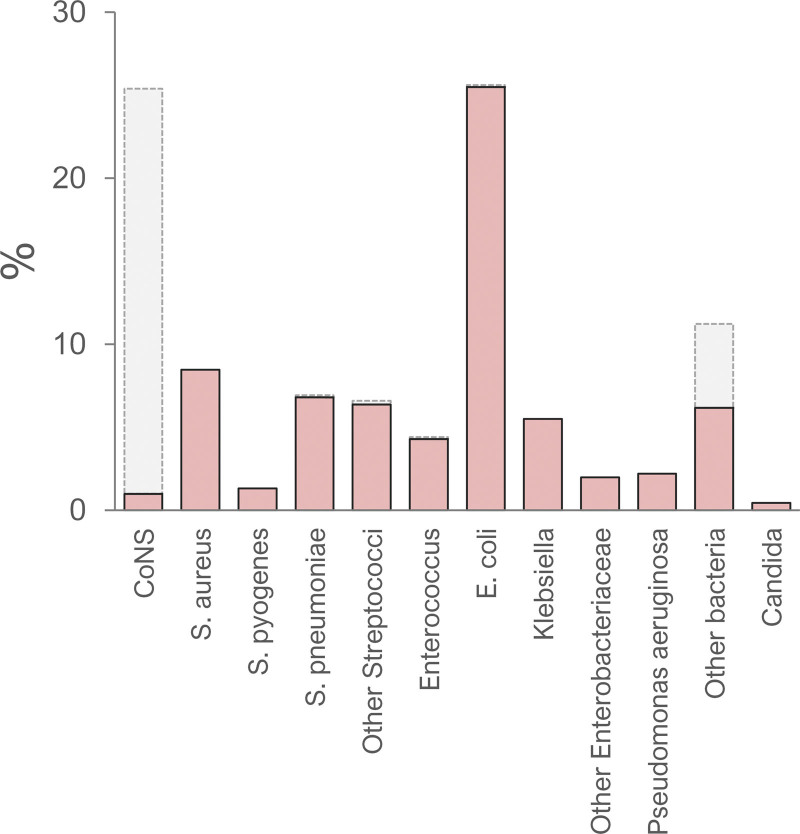
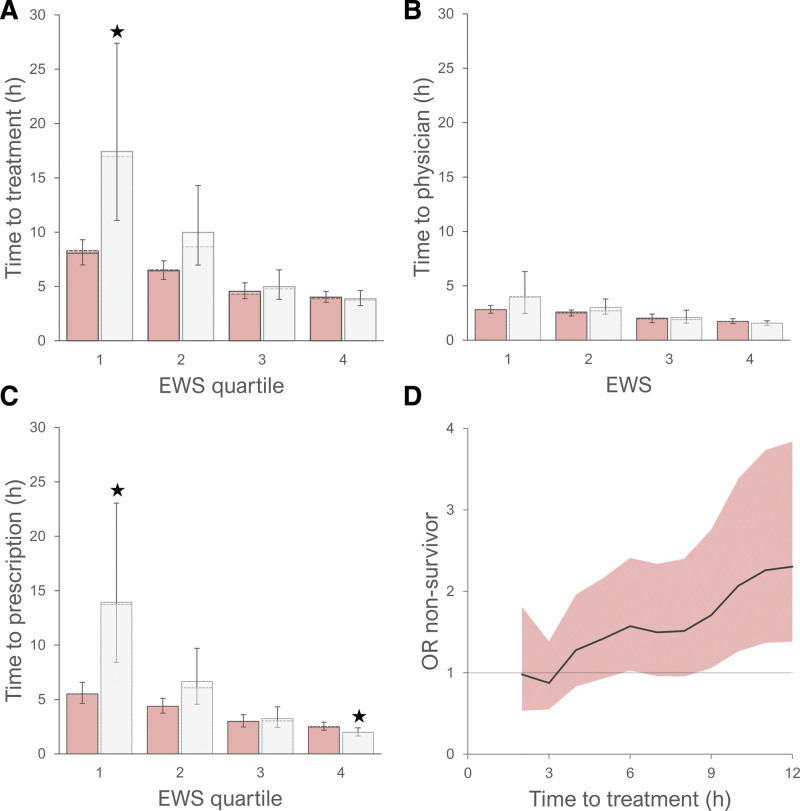
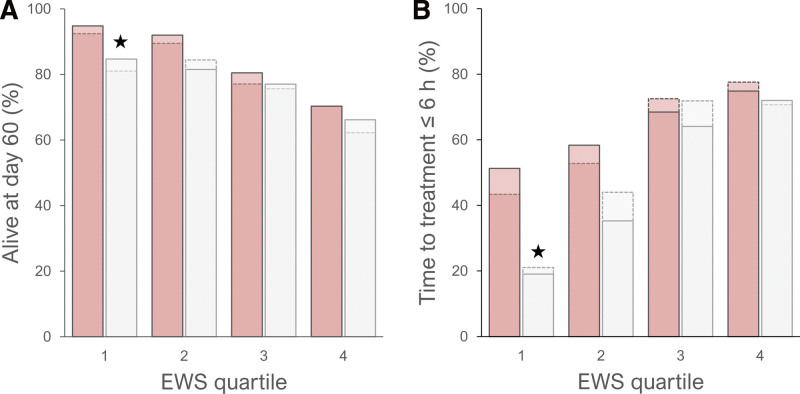
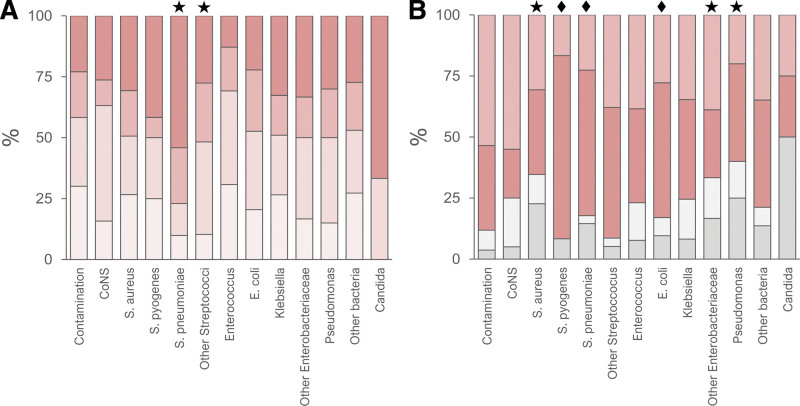
Measurements and main results: First recorded Early Warning Score (EWS), patient characteristics, time to antibiotic treatment, and survival at day 60 after admission were obtained from electronic health records and medicine module. Presence of contaminants and the match between the antibiotic treatment and susceptibility of the cultured microorganism were included in the analysis. Data were stratified according to EWS quartiles. Overall, time from admission to prescription of antibiotic treatment was 3.7 (3.4-4.0) hours, whereas time from admission to antibiotic treatment was 5.7 (5.4-6.1) hours. A gap between prescription and administration of antibiotic treatment was present across all EWS quartiles. Importantly, 23.4% of patients admitted with BSI presented with an initial EWS 0-1. Within this group of patients, time to antibiotic treatment was markedly higher among nonsurvivors at day 60 compared with survivors. Furthermore, time to antibiotic treatment later than 6 hours was associated with increased mortality at day 60. Among patients with an initial EWS of 0-1, 51.3% of survivors received antibiotic treatment within 6 hours, whereas only 19.0% of nonsurvivors received antibiotic treatment within 6 hours.
Conclusions: Among patients with initial low EWS, delay in antibiotic treatment of BSIs was associated with increased mortality at day 60. Lag from prescription to administration may contribute to delayed antibiotic treatment. A more frequent reevaluation of patients with infections with a low initial EWS and reduction of time from prescription to administration may reduce the time to antibiotic treatment, thus potentially improving survival.
Keywords: bacteremia; blood culture; organ dysfunction scores; systemic inflammatory response syndrome; triage.
Copyright © 2023 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Evans L, Rhodes A, Alhazzani W, et al. : Executive summary: Surviving sepsis campaign: International guidelines for the management of sepsis and septic shock 2021. Crit Care Med 2021; 49:1974–1982 - PubMed
-
- Kumar A, Roberts D, Wood KE, et al. : Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 2006; 34:1589–1596 - PubMed
-
- Puskarich MA, Trzeciak S, Shapiro NI, et al. ; Emergency Medicine Shock Research Network (EMSHOCKNET): Association between timing of antibiotic administration and mortality from septic shock in patients treated with a quantitative resuscitation protocol. Crit Care Med 2011; 39:2066–2071 - PMC - PubMed
-
- Ferrer R, Martin-Loeches I, Phillips G, et al. : Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: Results from a guideline-based performance improvement program. Crit Care Med 2014; 42:1749–1755 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
