

Multimodal Care of a Patient With Functional Movement Disorders Following a Motor Vehicle Accident: A Case Report
- PMID: 37644994
- PMCID: PMC10461147
- DOI: 10.1016/j.jcm.2023.03.010
Multimodal Care of a Patient With Functional Movement Disorders Following a Motor Vehicle Accident: A Case Report
Abstract
Objective: The purpose of this case report was to describe the multimodal care of a patient with the sudden onset of truncal tremors.
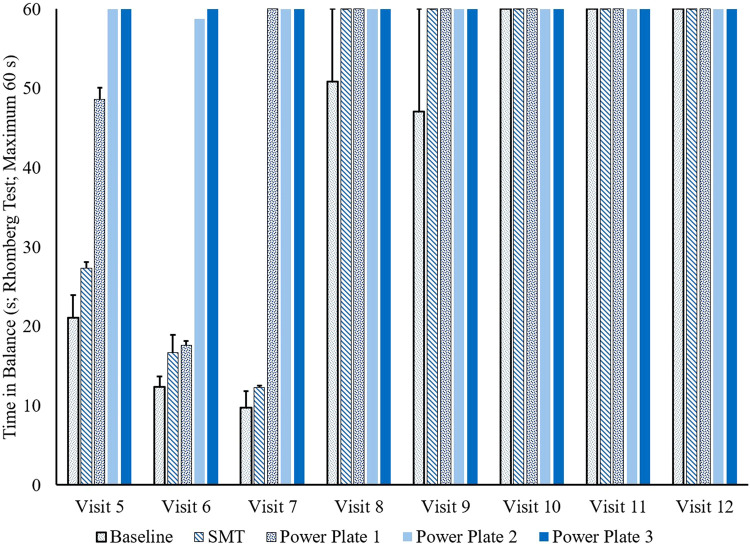
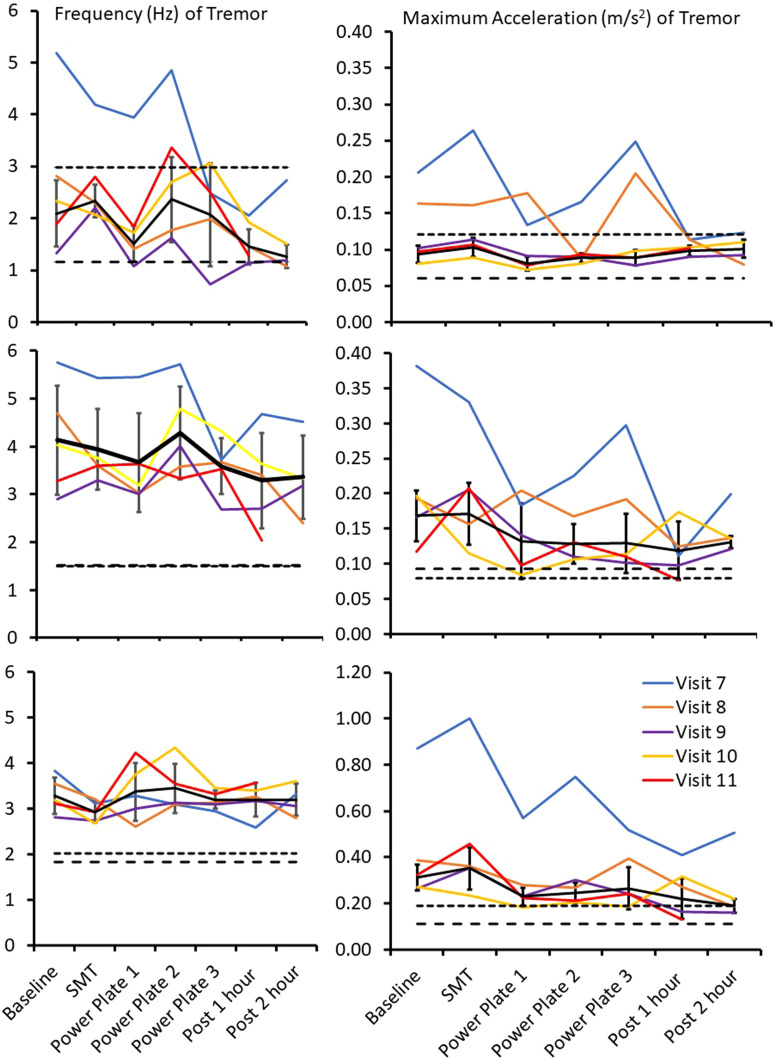
Clinical features: A 30-year-old female patient presented for chiropractic care with truncal tremors following a motor vehicle accident. Initial outcome measures included the Neck Disability Index (50%) and Oswestry Disability Index (62). The patient's truncal tremors became worse during spinal cord compression testing that included passive cervical flexion and slouched posture. The Romberg test was positive for swaying. Assessments of active range of motions of the cervical, thoracic, and lumbar spine were moderately reduced in all ranges. Case history, physical examinations, diagnostic imaging, and neurology consultations led to a diagnosis of functional truncal tremors. The patient was being concurrently managed by other health care providers. Magnetic resonance imaging studies were ordered by a neurologist and primary medical physician, which showed no structural abnormalities in brain neuroanatomy or spine.
Intervention and outcome: The multimodal chiropractic care included whole-body vibration therapy (WBVT), spinal manipulative therapy (SMT), and acupuncture therapy. The treatment plan included 8 weekly appointments in which the patient received WBVT and SMT. During treatment weeks 2 to 6, the patient received acupuncture therapy, which occurred immediately following their treatment appointment for WBVT and SMT. The patient practiced stress reduction techniques, as advised by the neurologist, eliminated caffeine, and performed daily yoga exercises for 30 minutes. The Romberg test was negative after the third treatment. The patient was discharged after chiropractic visit 12, 95 days post-accident, as she reached maximal medical improvement. Truncal tremors were still present, but the patient described them as "barely noticeable."
Conclusion: The patient reported improvement under a course of chiropractic care using a multimodal approach, including behavioral, pharmacological, and manual therapies. This case study suggests that WBVT, SMT, and acupuncture therapy may assist some patients with functional movement disorders.
Keywords: Acupuncture Therapy; Chiropractic; Psychosocial Intervention; Tremor; Vibration.
© 2023 by National University of Health Sciences.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
