

Ultrastructure for the diagnosis of primary ciliary dyskinesia in South Africa, a resource-limited setting
- PMID: 37645034
- PMCID: PMC10461090
- DOI: 10.3389/fped.2023.1247638
Ultrastructure for the diagnosis of primary ciliary dyskinesia in South Africa, a resource-limited setting
Abstract
Introduction: International guidelines recommend a multi-faceted approach for successful diagnoses of primary ciliary dyskinesia (PCD). In the absence of a gold standard test, a combination of genetic testing/microscopic analysis of structure and function/nasal nitric oxide measurement is used. In resource-limited settings, often none of the above tests are available, and in South Africa, only transmission electron microscopy (TEM) is available in central anatomical pathology departments. The aim of this study was to describe the clinical and ultrastructural findings of suspected PCD cases managed by pediatric pulmonologists at a tertiary-level state funded hospital in Johannesburg.
Methods: Nasal brushings were taken from 14 children with chronic respiratory symptoms in keeping with a PCD phenotype. Ultrastructural analysis in accordance with the international consensus guidelines for TEM-PCD diagnostic reporting was undertaken.
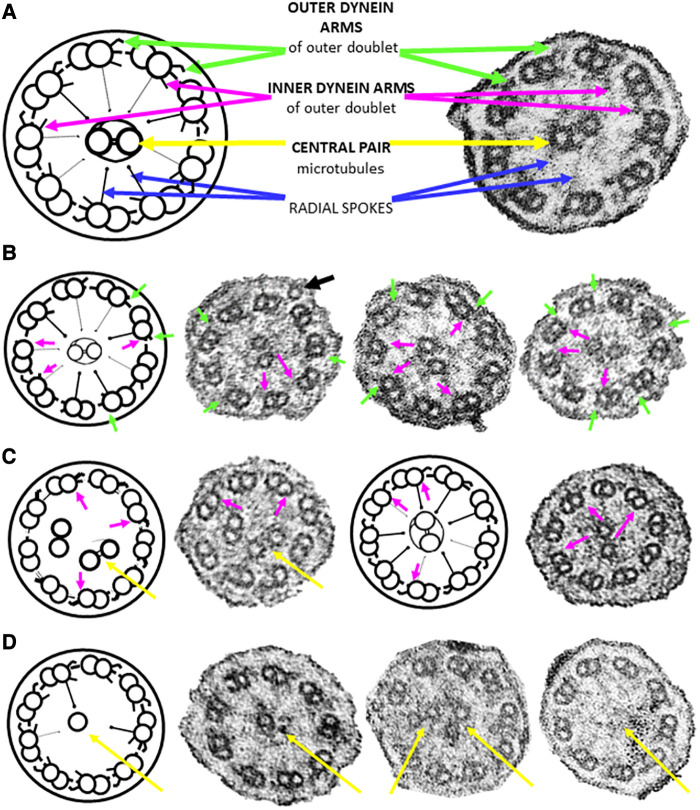
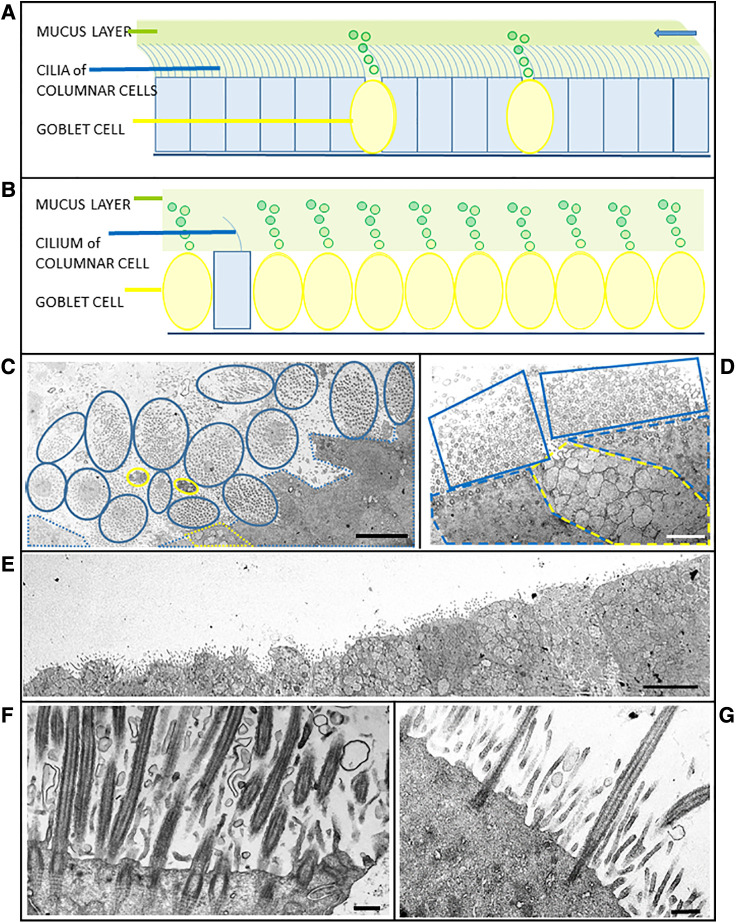
Results: TEM observations confirmed 43% (6) of the clinically-suspected cases (hallmark ultrastructural defects in the dynein arms of the outer doublets), whilst 57% (8) required another PCD testing modality to support ultrastructural observations. Of these, 25% (2) had neither ultrastructural defects nor did they present with bronchiectasis. Of the remaining cases, 83% (5) had very few ciliated cells (all of which were sparsely ciliated), together with goblet cell hyperplasia. There was the apparent absence of ciliary rootlets in 17% (1) case.
Discussion: In resource-limited settings in which TEM is the only available testing modality, confirmatory and probable diagnoses of PCD can be made to facilitate early initiation of treatment of children with chronic respiratory symptoms.
Keywords: South Africa; clinical phenotype; primary ciliary dyskinesia; resource-limited; ultrastructure (electron microscopy).
© 2023 Birkhead, Otido, Mabaso, Mopeli, Tlhapi, Verwey and Dangor.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- O’Connor MG, Mosquera R, Metjian H, Marmor M, Olivier KN, Shapiro AJ. Primary ciliary dyskinesia. Chest Pulmonary. (2023) 1:100004. 10.1016/j.chpulm.2023.100004 - DOI
LinkOut - more resources
Full Text Sources