

Adding Tibial Tuberosity Medialization to Medial Patellofemoral Ligament Reconstruction Reduces Lateral Patellar Maltracking During Multidirectional Motion in a Computational Simulation Model
- PMID: 37645404
- PMCID: PMC10461214
- DOI: 10.1016/j.asmr.2023.100753
Adding Tibial Tuberosity Medialization to Medial Patellofemoral Ligament Reconstruction Reduces Lateral Patellar Maltracking During Multidirectional Motion in a Computational Simulation Model
Abstract
Purpose: To determine whether adding tibial tuberosity medialization to medial patellofemoral ligament (MPFL) reconstruction reduces lateral patellar maltracking during a dynamic multidirectional activity and to investigate when medial patellofemoral contact pressures are elevated during daily activities, such as squatting.
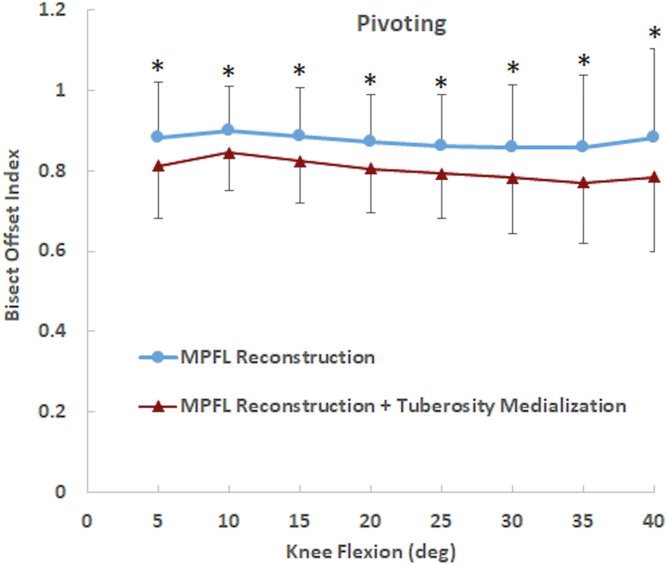
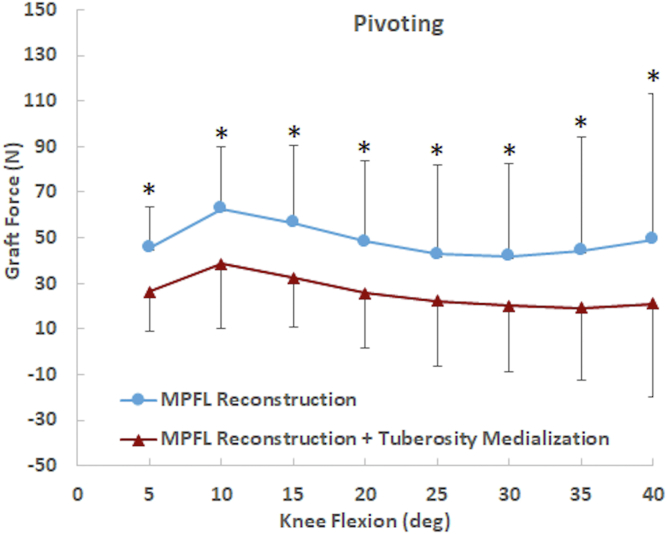
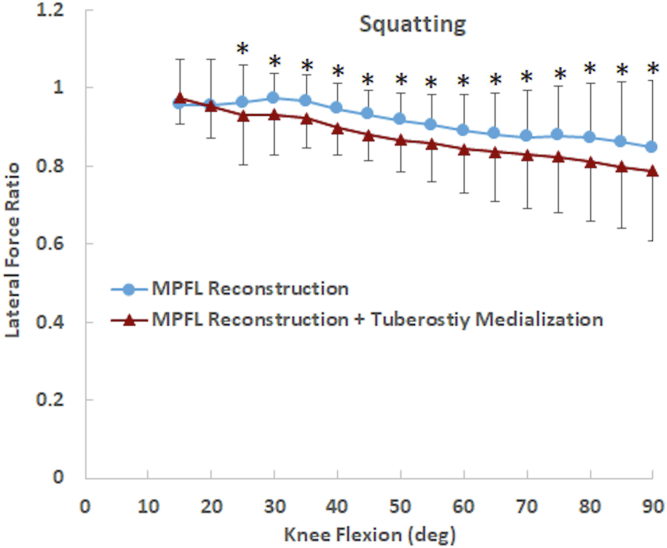
Methods: Seven computational models representing knees with patellar instability, including lateral patellar maltracking, were evaluated following simulated MPFL reconstruction (bisect offset index > .75). Tibial tuberosity medialization was added to MPFL reconstruction for each model. Patellar tracking during multidirectional motion was evaluated by simulating pivot landing. Analysis of pivoting focused on early flexion (5° to 40°). Patellofemoral contact pressures during daily function were evaluated by simulating knee squatting. Data were analyzed with paired comparisons between MPFL reconstruction with and without tuberosity medialization.
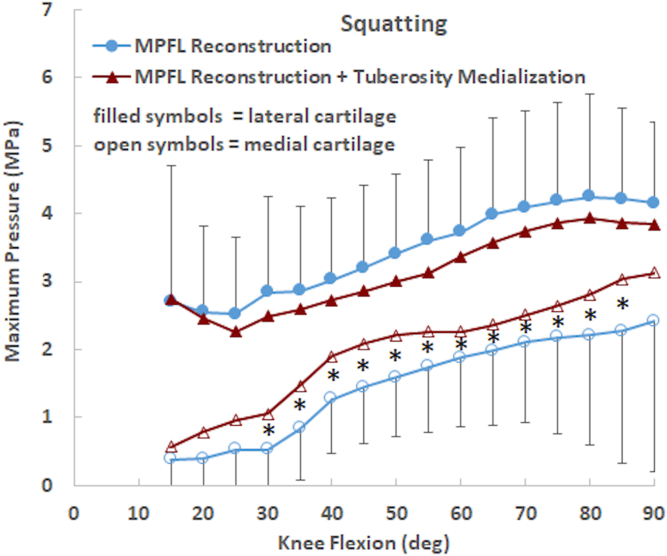
Results: The patella dislocated during pivoting for 2 models with an isolated MPFL reconstruction and for 1 model including tibial tuberosity medialization. Adding tibial tuberosity medialization to MPFL reconstruction significantly decreased bisect offset index by ∼0.1 from 5° to 40° (P < .03). For knee squatting, medializing the tibial tuberosity significantly increased maximum medial contract pressure by ∼0.5 MPa from 30° to 85° (P < .05) but did not significantly influence maximum lateral pressure.
Conclusions: In this study of simulated multidirectional motion, MPFL reconstruction did not sufficiently constrain the patella for some knees. Adding tibial tuberosity medialization to MPFL reconstruction in these models reduced lateral patellar maltracking during multidirectional motion but increased pressure applied to medial cartilage during squatting.
Clinical relevance: After establishing the influence of tibial tuberosity medialization on patellar maltracking for an idealized population, as was done in the current study, future simulation studies can be performed to better determine the anatomical characteristics of patients for whom tibial tuberosity medialization is needed to reduce the risk of postoperative patellar maltracking.
© 2023 The Authors.
Figures


Similar articles
-
Computational simulation of medial versus anteromedial tibial tuberosity transfer for patellar instability.J Orthop Res. 2018 Dec;36(12):3231-3238. doi: 10.1002/jor.24108. Epub 2018 Aug 2. J Orthop Res. 2018. PMID: 30024053 Free PMC article.
-
Dynamic tracking influenced by anatomy following medial patellofemoral ligament reconstruction: Computational simulation.Knee. 2018 Mar;25(2):262-270. doi: 10.1016/j.knee.2018.02.002. Epub 2018 Mar 13. Knee. 2018. PMID: 29544985 Free PMC article.
-
Tibial tuberosity anteriomedialization vs. medial patellofemoral ligament reconstruction for treatment of patellar instability related to malalignment: Computational simulation.Clin Biomech (Bristol). 2020 Apr;74:111-117. doi: 10.1016/j.clinbiomech.2020.01.019. Epub 2020 Jan 30. Clin Biomech (Bristol). 2020. PMID: 32171152 Free PMC article.
-
Biomechanical Analysis of Tibial Tuberosity Medialization and Medial Patellofemoral Ligament Reconstruction.Sports Med Arthrosc Rev. 2017 Jun;25(2):58-63. doi: 10.1097/JSA.0000000000000152. Sports Med Arthrosc Rev. 2017. PMID: 28459747 Free PMC article. Review.
-
Inconsistencies in Reporting Risk Factors for Medial Patellofemoral Ligament Reconstruction Failure: A Systematic Review.Am J Sports Med. 2022 Mar;50(3):867-877. doi: 10.1177/03635465211003342. Epub 2021 Apr 29. Am J Sports Med. 2022. PMID: 33914648
Cited by
-
Medial Quadriceps Tendon Femoral Ligament Reconstruction for Recurrent Patellar Instability in Skeletal Immature Patients Using Anterior Tibialis Tendon Allograft.Arthrosc Tech. 2025 May 29;14(7):103630. doi: 10.1016/j.eats.2025.103630. eCollection 2025 Jul. Arthrosc Tech. 2025. PMID: 40822180 Free PMC article.
References
-
- Liu J.N., Steinhaus M.E., Kalbian I.L., et al. Patellar instability management: A survey of the International Patellofemoral Study Group. Am J Sports Med. 2018;46:3299–3306. - PubMed
-
- Hopper G.P., Leach W.J., Rooney B.P., Walker C.R., Blyth M.J. Does degree of trochlear dysplasia and position of femoral tunnel influence outcome after medial patellofemoral ligament reconstruction? Am J Sports Med. 2014;42:716–722. - PubMed
-
- Hiemstra L.A., Kerslake S., Loewen M., Lafave M. Effect of trochlear dysplasia on outcomes after isolated soft tissue stabilization for patellar instability. Am J Sports Med. 2016;44:1515–1523. - PubMed
-
- Kita K., Tanaka Y., Toritsuka Y., et al. Factors affecting the outcomes of double-bundle medial patellofemoral ligament reconstruction for recurrent patellar dislocations evaluated by multivariate analysis. Am J Sports Med. 2015;43:2988–2996. - PubMed
LinkOut - more resources
Full Text Sources
