

High baseline frequencies of natural killer cells are associated with asymptomatic SARS-CoV-2 infection
- PMID: 37645658
- PMCID: PMC10461189
- DOI: 10.1016/j.crimmu.2023.100064
High baseline frequencies of natural killer cells are associated with asymptomatic SARS-CoV-2 infection
Abstract
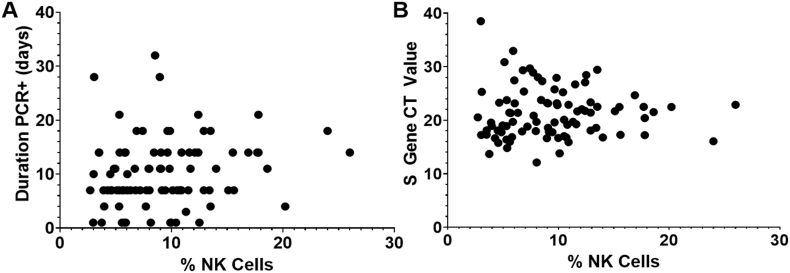
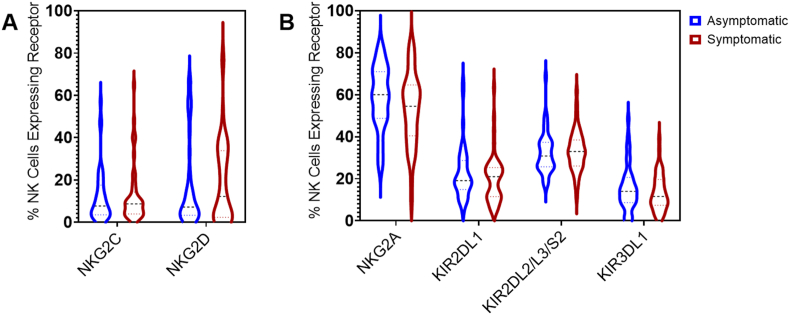
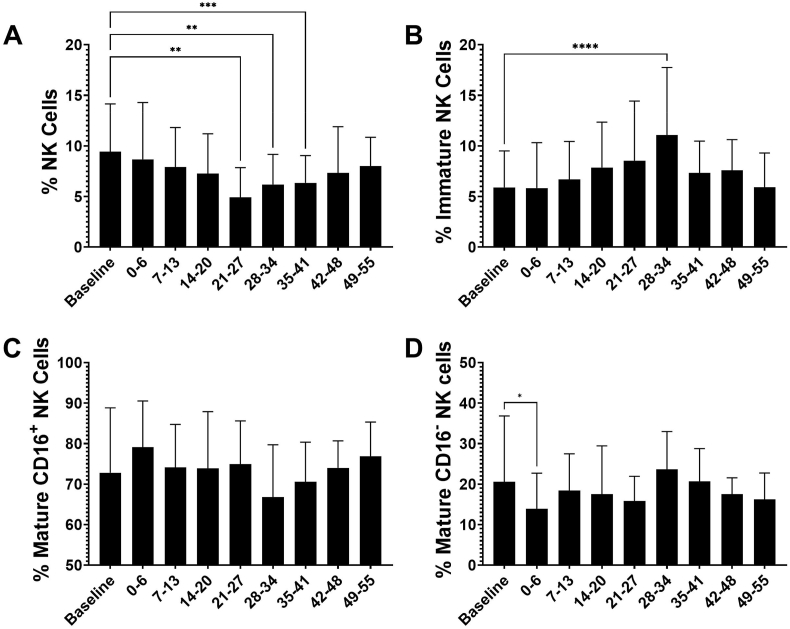
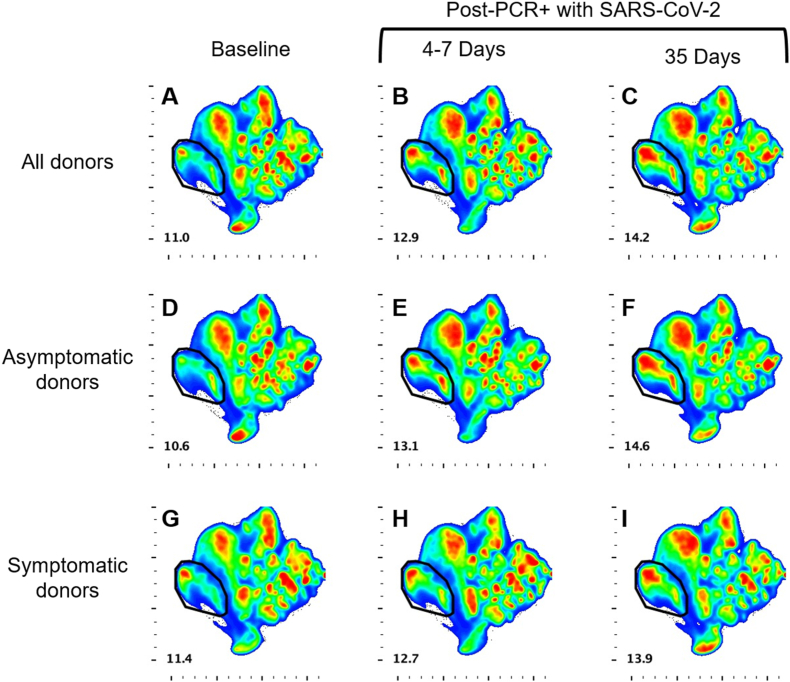
This study tested the hypothesis that high frequencies of natural killer (NK) cells are protective against symptomatic SARS-CoV-2 infection. Samples were utilized from the COVID-19 Health Action Response for Marines study, a prospective, observational study of SARS-CoV-2 infection in which participants were enrolled prior to infection and then serially monitored for development of symptomatic or asymptomatic infection. Frequencies and phenotypes of NK cells (CD3-CD14-CD19-CD56+) were assessed by flow cytometry. Individuals that developed asymptomatic infections were found to have higher pre-infection frequencies of total NK cells compared to symptomatic individuals (10.61% [SD 4.5] vs 8.33% [SD 4.6], p = 0.011). Circulating total NK cells decreased over the course of infection, reaching a nadir at 4 weeks, while immature NK cells increased, a finding confirmed by multidimensional reduction analysis. These results indicate that NK cells likely play a key role in controlling the severity of clinical illness in individuals infected with SARS-CoV-2.
Keywords: Asymptomatic; NK cells; Natural killer cells; SARS-CoV-2; Symptomatic.
© 2023 Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Uniformed Services University of the Health Sciences, Department of the Navy, Department of Defense, the U.S. Government, nor the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. AMWM, PS, SL, RL, DLW, CWG, AGL, and EM are military Service members or employees of the U.S. Government. This work was prepared as part of their official duties. Title 17, U.S.C., §105 provides that copyright protection under this title is not available for any work of the U.S. Government. Title 17, U.S.C., §101 defines a U.S. Government work as a work prepared by a military Service member or employee of the U.S. Government as part of that person’s official duties.
Figures


References
-
- Béziat V., Liu L.L., Malmberg J.A., Ivarsson M.A., Sohlberg E., Björklund A.T., Retière C., Sverremark-Ekström E., Traherne J., Ljungman P., Schaffer M., Price D.A., Trowsdale J., Michaëlsson J., Ljunggren H.G., Malmberg K.J. NK cell responses to cytomegalovirus infection lead to stable imprints in the human KIR repertoire and involve activating KIRs. Blood. 2013;121:2678–2688. - PMC - PubMed
-
- Bozzano F., Dentone C., Perrone C., Di Biagio A., Fenoglio D., Parodi A., Mikulska M., Bruzzone B., Giacobbe D.R., Vena A., Taramasso L., Nicolini L., Patroniti N., Pelosi P., Gratarola A., De Palma R., Filaci G., Bassetti M., De Maria A. Extensive activation, tissue trafficking, turnover and functional impairment of NK cells in COVID-19 patients at disease onset associates with subsequent disease severity. PLoS Pathog. 2021;17 - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
