

This is a preprint.
Timing dependent synergies between motor cortex and posterior spinal stimulation in humans
- PMID: 37645795
- PMCID: PMC10462218
- DOI: 10.1101/2023.08.18.23294259
Timing dependent synergies between motor cortex and posterior spinal stimulation in humans
Update in
-
Timing-dependent synergies between motor cortex and posterior spinal stimulation in humans.J Physiol. 2024 Jun;602(12):2961-2983. doi: 10.1113/JP286183. Epub 2024 May 17. J Physiol. 2024. PMID: 38758005 Free PMC article.
Abstract
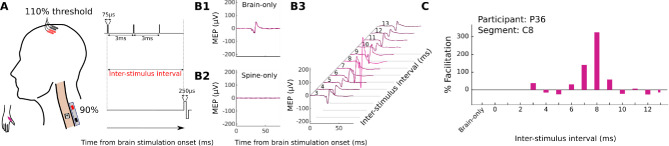
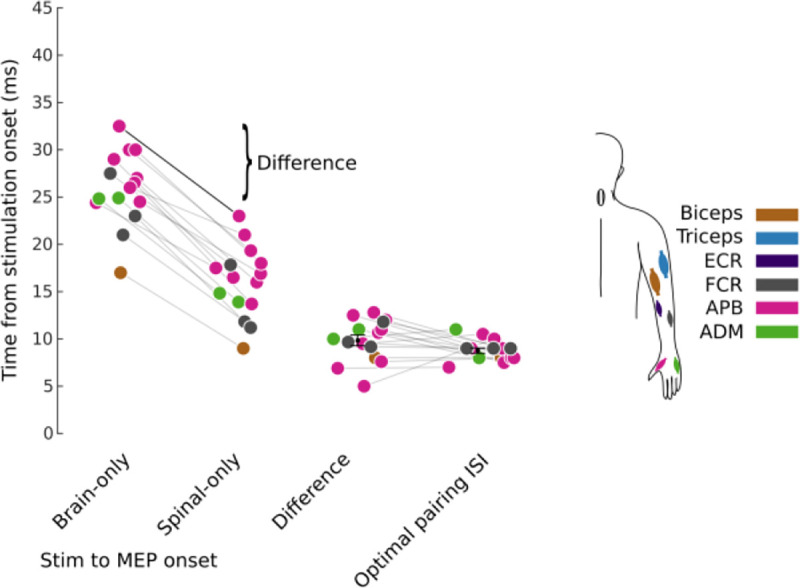
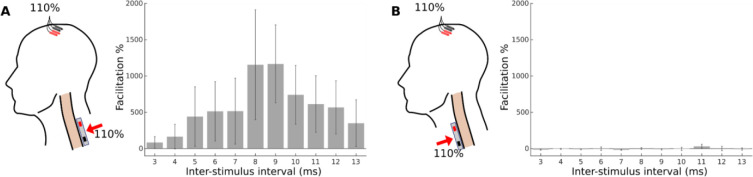
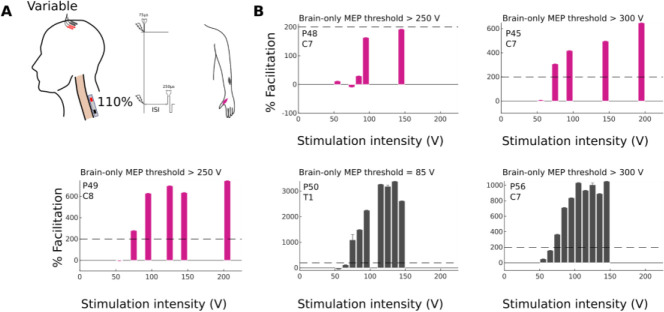
Volitional movement requires descending input from motor cortex and sensory feedback through the spinal cord. We previously developed a paired brain and spinal electrical stimulation approach in rats that relies on convergence of the descending motor and spinal sensory stimuli in the cervical cord. This approach strengthened sensorimotor circuits and improved volitional movement through associative plasticity. In humans it is not known whether dorsal epidural SCS targeted at the sensorimotor interface or anterior epidural SCS targeted within the motor system is effective at facilitating brain evoked responses. In 59 individuals undergoing elective cervical spine decompression surgery, the motor cortex was stimulated with scalp electrodes and the spinal cord with epidural electrodes while muscle responses were recorded in arm and leg muscles. Spinal electrodes were placed either posteriorly or anteriorly, and the interval between cortex and spinal cord stimulation was varied. Pairing stimulation between the motor cortex and spinal sensory (posterior) but not spinal motor (anterior) stimulation produced motor evoked potentials that were over five times larger than brain stimulation alone. This strong augmentation occurred only when descending motor and spinal afferent stimuli were timed to converge in the spinal cord. Paired stimulation also increased the selectivity of muscle responses relative to unpaired brain or spinal cord stimulation. Finally, paired stimulation effects were present regardless of the severity of myelopathy as measured by clinical signs or spinal cord imaging. The large effect size of this paired stimulation makes it a promising candidate for therapeutic neuromodulation.
Keywords: Cervical; Electrical stimulation; Epidural; Motor cortex; Motor evoked potentials; Myelopathy; Spinal cord.
Conflict of interest statement
5.1Competing interests Jason B. Carmel is a Founder and stock holder in BackStop Neural and a scientific advisor and stockholder in SharperSense. He has received honoraria from Pacira, Motric Bio, and Restorative Therapeutics. Michael S. Virk has been a consultant and has received honorarium from Depuy Synthes and BrainLab Inc; he is on the Medical Advisory Board and owns stock with OnPoint Surgical. K. Daniel Riew: Consulting: Happe Spine (Nonfinancial), Nuvasive; Royalties: Biomet, Nuvasive; Speaking and/or Teaching Arrangements: Nuvasive (Travel Expense Reimbursement); Stock Ownership: Amedica, Axiomed, Benvenue, Expanding Orthopedics, Happe Spine, Paradigm Spine, Spinal Kinetics, Spineology, Vertiflex. Ronald A. Lehman: Consulting: Medtronic; Royalties: Medtronic, Stryker. Zeeshan M. Sardar: Consulting: Medtronic; Grant/Research support from the Department of Defense. Joseph M. Lombardi: Consulting: Medtronic, Stryker. The other authors have nothing to disclose.
Figures







References
-
- Al’joboori Yazi, Hannah Ricci, Lenham Francesca, Borgas Pia, Kremers Charlotte J. P., Bunday Karen L., Rothwell John, and Duffell Lynsey D.. 2021. “The Immediate and Short-Term Effects of Transcutaneous Spinal Cord Stimulation and Peripheral Nerve Stimulation on Corticospinal Excitability.” Frontiers in Neuroscience 15. 10.3389/fnins.2021.749042. - DOI - PMC - PubMed
-
- Angeli Claudia A., Boakye Maxwell, Morton Rebekah A., Vogt Justin, Benton Kristin, Chen Yangshen, Ferreira Christie K., and Harkema Susan J.. 2018. “Recovery of Over-Ground Walking after Chronic Motor Complete Spinal Cord Injury.” New England Journal of Medicine 379 (13): 1244–50. 10.1056/NEJMoa1803588. - DOI - PubMed
-
- Benzel Edward C., Lancon John, Kesterson Lee, and Hadden Theresa. 1991. “Cervical Laminectomy and Dentate Ligament Section for Cervical Spondylotic Myelopathy.” Clinical Spine Surgery 4 (3): 286. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources