

Deep learning for risk-based stratification of cognitively impaired individuals
- PMID: 37646016
- PMCID: PMC10460987
- DOI: 10.1016/j.isci.2023.107522
Deep learning for risk-based stratification of cognitively impaired individuals
Abstract
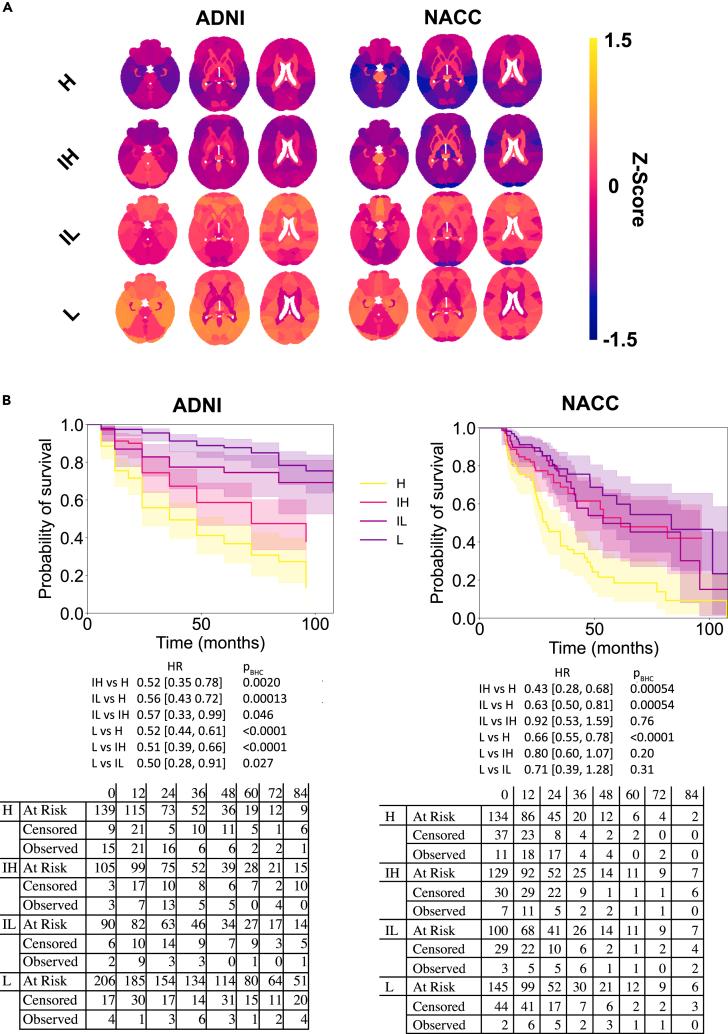
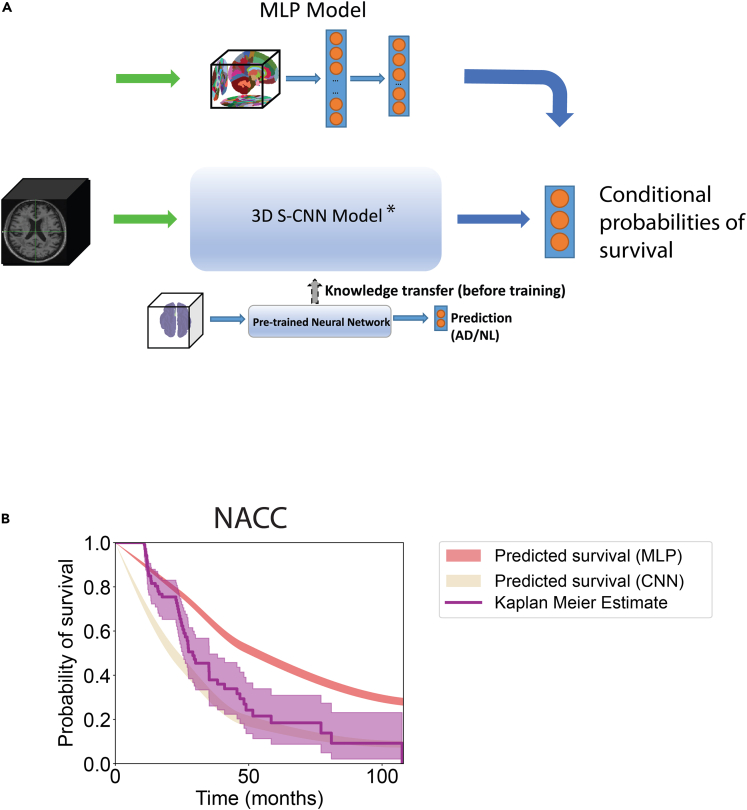
Quantifying the risk of progression to Alzheimer's disease (AD) could help identify persons who could benefit from early interventions. We used data from the Alzheimer's Disease Neuroimaging Initiative (ADNI, n = 544, discovery cohort) and the National Alzheimer's Coordinating Center (NACC, n = 508, validation cohort), subdividing individuals with mild cognitive impairment (MCI) into risk groups based on cerebrospinal fluid amyloid-β levels and identifying differential gray matter patterns. We then created models that fused neural networks with survival analysis, trained using non-parcellated T1-weighted brain MRIs from ADNI data, to predict the trajectories of MCI to AD conversion within the NACC cohort (integrated Brier score: 0.192 [discovery], and 0.108 [validation]). Using modern interpretability techniques, we verified that regions important for model prediction are classically associated with AD. We confirmed AD diagnosis labels using postmortem data. We conclude that our framework provides a strategy for risk-based stratification of individuals with MCI and for identifying regions key for disease prognosis.
Keywords: Health sciences; Illness behavior.
© 2023 The Author(s).
Conflict of interest statement
V.B.K. reports honoraria from invited scientific presentations not exceeding $5000/year. He also serves as a consultant to Davos Alzheimer’s Collaborative and AstraZeneca. R.A. is a scientific advisor to Signant Health and consultant to Biogen. The remaining authors declare no competing interests.
Figures





References
-
- Schneider L.S., Mangialasche F., Andreasen N., Feldman H., Giacobini E., Jones R., Mantua V., Mecocci P., Pani L., Winblad B., Kivipelto M. Clinical trials and late-stage drug development for Alzheimer's disease: an appraisal from 1984 to 2014. J. Intern. Med. 2014;275:251–283. doi: 10.1111/joim.12191. - DOI - PMC - PubMed
