

Predicting poor neurological outcomes following out-of-hospital cardiac arrest using neuron-specific enolase and neurofilament light chain in patients with and without haemolysis
- PMID: 37646044
- PMCID: PMC10461601
- DOI: 10.1093/ehjopen/oead078
Predicting poor neurological outcomes following out-of-hospital cardiac arrest using neuron-specific enolase and neurofilament light chain in patients with and without haemolysis
Abstract
Aims: Hypoxic-ischaemic brain injury following out-of-hospital cardiac arrest (OHCA) is a common complication and a major cause of death. Neuron-specific enolase (NSE) and neurofilament light chain (NfL) are released after brain injury and elevated concentrations of both are associated with poor neurological outcome. We explored the influence of haemolysis on the prognostic performance of NSE and NfL.
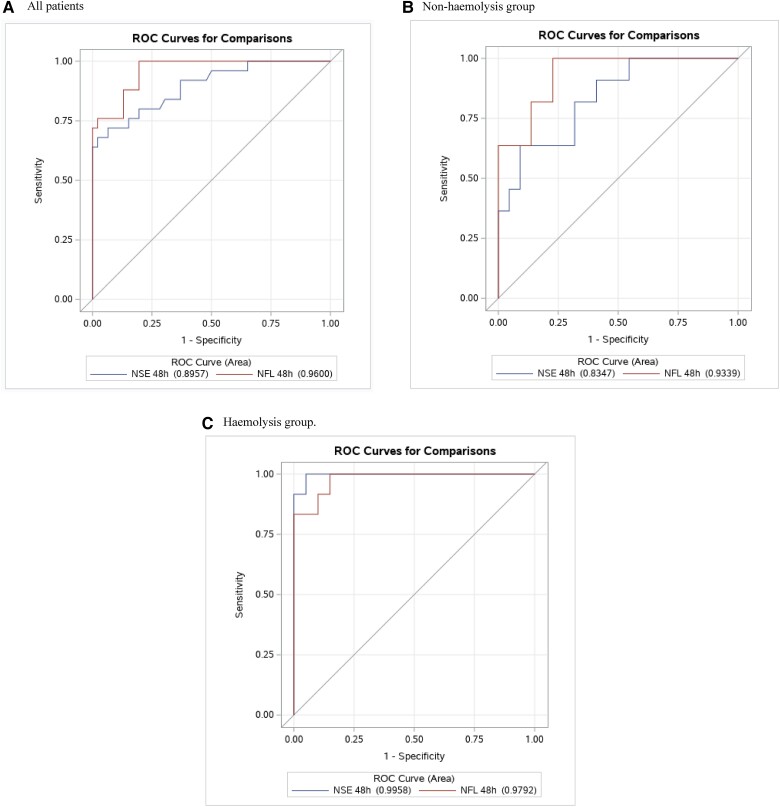
Methods and results: The study is based on post hoc analyses of a randomized, single-centre, double-blinded, controlled trial (IMICA), where comatose OHCA patients of presumed cardiac cause were included. Free-haemoglobin was measured at admission to quantify haemolysis. NSE and NfL were measured after 48 h to estimate the extent of brain injury. Montreal Cognitive Assessment score (MoCA) was assessed to evaluate neurocognitive impairments. Seventy-three patients were included and divided into two groups by the median free-haemoglobin at admission. No group differences in mortality or poor neurological outcome were observed. The high-admission free-haemoglobin group had a significantly higher concentration of NSE compared to the low-admission free-haemoglobin group (27.4 µmol/L vs. 19.6 µmol/L, P = 0.03), but no differences in NfL. The performance of NSE and NfL in predicting poor neurological outcome were high for both, but NfL was numerically higher [area under the ROC (AUROC) 0.90 vs. 0.96, P = 0.09]. Furthermore, NfL, but not NSE, was inversely correlated with MoCA score, R2 = 0.21, P = 0.006.
Conclusion: High free-haemoglobin at admission was associated with higher NSE concentration after 48 h, but, the performance of NSE and NfL in predicting poor neurological outcome among OHCA patients were good regardless of early haemolysis. Only elevated NfL concentrations were associated with cognitive impairments.
Keywords: Free-haemoglobin; Haemolysis; MoCA; Neurofilament light chain; Neuron-specific enolase; Out-of-hospital cardiac arrest.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflicts of interest: All authors declare no conflict of interest except Anna Sina Petterson Meyer which has been employed at Novo Nordisk after the completion of the trial.
Figures
Similar articles
-
Neurofilament Light Chain and Glial Fibrillary Acidic Protein as early prognostic biomarkers after out-of-hospital cardiac arrest.Resuscitation. 2023 Dec;193:109983. doi: 10.1016/j.resuscitation.2023.109983. Epub 2023 Sep 29. Resuscitation. 2023. PMID: 37778613
-
Neurofilament light compared to neuron-specific enolase as a predictor of unfavourable outcome after out-of-hospital cardiac arrest.Resuscitation. 2022 May;174:1-8. doi: 10.1016/j.resuscitation.2022.02.024. Epub 2022 Mar 1. Resuscitation. 2022. PMID: 35245610
-
Predicting neurological outcome after out-of-hospital cardiac arrest with cumulative information; development and internal validation of an artificial neural network algorithm.Crit Care. 2021 Feb 25;25(1):83. doi: 10.1186/s13054-021-03505-9. Crit Care. 2021. PMID: 33632280 Free PMC article.
-
Serum neurofilament light chain as a predictive marker of neurologic outcome after cardiac arrest: a meta-analysis.BMC Cardiovasc Disord. 2023 Apr 15;23(1):193. doi: 10.1186/s12872-023-03220-z. BMC Cardiovasc Disord. 2023. PMID: 37061702 Free PMC article.
-
Neuroprognostication value of serum neurofilament light chain for out-of-hospital cardiac arrest: A systematic review and meta-analysis.PLoS One. 2023 Sep 15;18(9):e0290619. doi: 10.1371/journal.pone.0290619. eCollection 2023. PLoS One. 2023. PMID: 37713399 Free PMC article.
Cited by
-
Neurofilament light chain for prognostication after cardiac arrest-first steps towards validation.Crit Care. 2025 Aug 6;29(1):348. doi: 10.1186/s13054-025-05579-1. Crit Care. 2025. PMID: 40770665 Free PMC article. Clinical Trial.
-
Predictive Performance of Neuron-Specific Enolase (NSE) for Survival after Resuscitation from Cardiac Arrest: A Systematic Review and Meta-Analysis.J Clin Med. 2023 Dec 13;12(24):7655. doi: 10.3390/jcm12247655. J Clin Med. 2023. PMID: 38137724 Free PMC article. Review.
References
-
- Lemiale V, Dumas F, Mongardon N, Giovanetti O, Charpentier J, Chiche JD, Carli P, Mira JP, Nolan J, Cariou A. Intensive care unit mortality after cardiac arrest: the relative contribution of shock and brain injury in a large cohort. Intensive Care Med 2013;39:1972–1980. - PubMed
-
- Sendelbach S, Hearst MO, Johnson PJ, Unger BT, Mooney MR. Effects of variation in temperature management on cerebral performance category scores in patients who received therapeutic hypothermia post cardiac arrest. Resuscitation 2012;83:829–834. - PubMed
-
- Nolan JP, Neumar RW, Adrie C, Aibiki M, Berg RA, Böttiger BW, Callaway C, Clark RS, Geocadin RG, Jauch EC, Kern KB, Laurent I, Longstreth WT, Merchant RM, Morley P, Morrison LJ, Nadkarni V, Peberdy MA, Rivers EP, Rodriguez-Nunez A, Sellke FW, Spaulding C, Sunde K, Hoek TV. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A scientific statement from the international liaison committee on resuscitation; the American heart association emergency cardiovascular care committee; the council on cardiovascular surgery and anesthesia; the council on cardiopulmonary, perioperative, and critical care; the council on clinical cardiology; the council on stroke. Resuscitation 2008;79:350–379. - PubMed
LinkOut - more resources
Full Text Sources
