

Stroke risk in women with atrial fibrillation
- PMID: 37647629
- PMCID: PMC10771362
- DOI: 10.1093/eurheartj/ehad508
Stroke risk in women with atrial fibrillation
Abstract
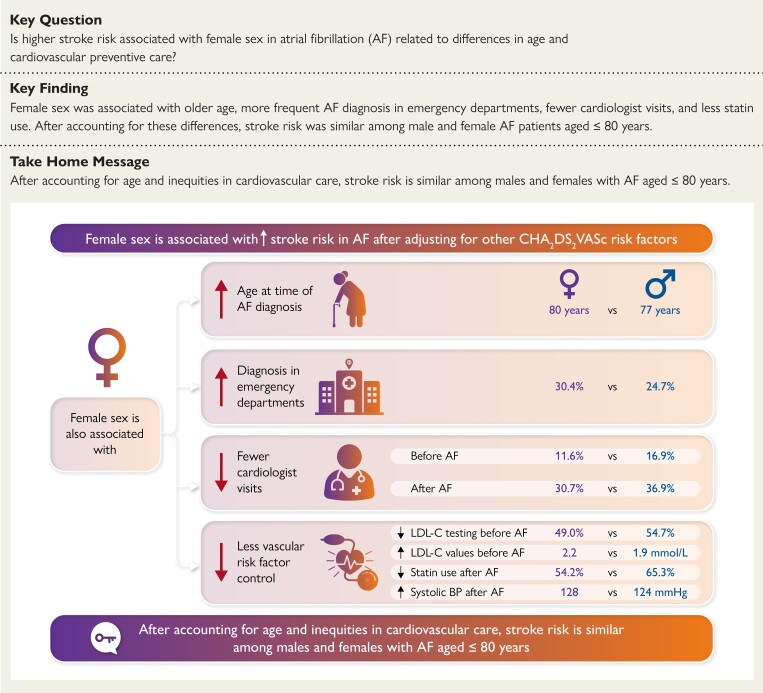
Background and aims: Female sex is associated with higher rates of stroke in atrial fibrillation (AF) after adjustment for other CHA2DS2-VASc factors. This study aimed to describe sex differences in age and cardiovascular care to examine their relationship with stroke hazard in AF.
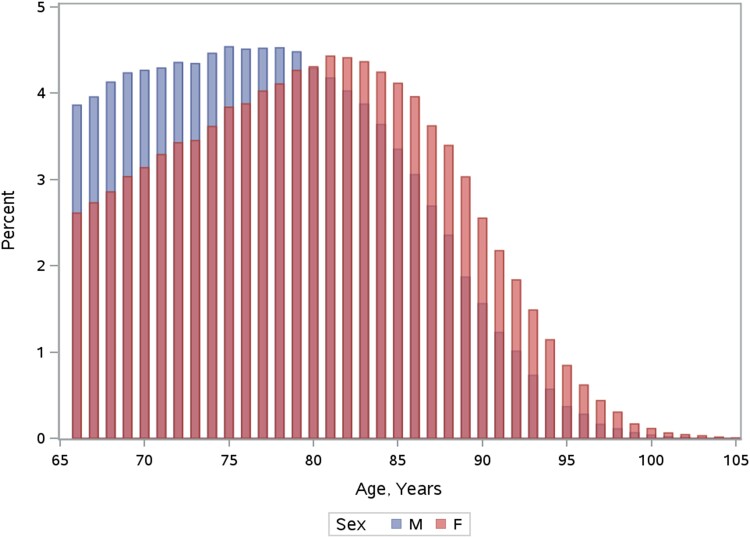
Methods: Population-based cohort study using administrative datasets of people aged ≥66 years diagnosed with AF in Ontario between 2007 and 2019. Cause-specific hazard regression was used to estimate the adjusted hazard ratio (HR) for stroke associated with female sex over a 2-year follow-up. Model 1 included CHA2DS2-VASc factors, with age modelled as 66-74 vs. ≥ 75 years. Model 2 treated age as a continuous variable and included an age-sex interaction term. Model 3 further accounted for multimorbidity and markers of cardiovascular care.
Results: The cohort consisted of 354 254 individuals with AF (median age 78 years, 49.2% female). Females were more likely to be diagnosed in emergency departments and less likely to receive cardiologist assessments, statins, or LDL-C testing, with higher LDL-C levels among females than males. In Model 1, the adjusted HR for stroke associated with female sex was 1.27 (95% confidence interval 1.21-1.32). Model 2 revealed a significant age-sex interaction, such that female sex was only associated with increased stroke hazard at age >70 years. Adjusting for markers of cardiovascular care and multimorbidity further decreased the HR, so that female sex was not associated with increased stroke hazard at age ≤80 years.
Conclusion: Older age and inequities in cardiovascular care may partly explain higher stroke rates in females with AF.
Keywords: Atrial Fibrillation; Female sex; Stroke.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures


Comment in
-
The stroke enigma: decoding the sex risk factor in atrial fibrillation.Eur Heart J. 2024 Jan 7;45(2):114-116. doi: 10.1093/eurheartj/ehad531. Eur Heart J. 2024. PMID: 37670405 No abstract available.
References
-
- Abdel-Qadir H, Singh SM, Pang A, Austin PC, Jackevicius CA, Tu K, et al. Evaluation of the risk of stroke without anticoagulation therapy in men and women with atrial fibrillation aged 66 to 74 years without other CHA2DS2-VASc factors. JAMA Cardiol 2021;6:918–25. 10.1001/jamacardio.2021.1232 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
