

Sorafenib plus intensive chemotherapy in newly diagnosed FLT3-ITD AML: a randomized, placebo-controlled study by the ALLG
- PMID: 37647654
- PMCID: PMC10733823
- DOI: 10.1182/blood.2023020301
Sorafenib plus intensive chemotherapy in newly diagnosed FLT3-ITD AML: a randomized, placebo-controlled study by the ALLG
Abstract
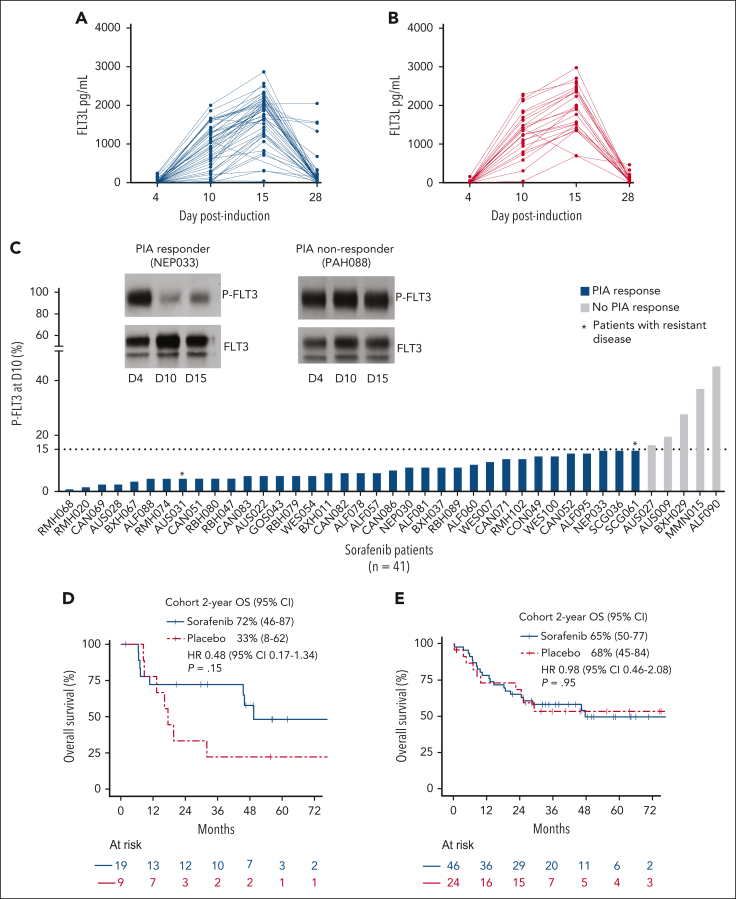
Sorafenib maintenance improves outcomes after hematopoietic cell transplant (HCT) for patients with FMS-like tyrosine kinase 3-internal tandem duplication (FLT3-ITD) acute myeloid leukemia (AML). Although promising outcomes have been reported for sorafenib plus intensive chemotherapy, randomized data are limited. This placebo-controlled, phase 2 study (ACTRN12611001112954) randomized 102 patients (aged 18-65 years) 2:1 to sorafenib vs placebo (days 4-10) combined with intensive induction: idarubicin 12 mg/m2 on days 1 to 3 plus either cytarabine 1.5 g/m2 twice daily on days 1, 3, 5, and 7 (18-55 years) or 100 mg/m2 on days 1 to 7 (56-65 years), followed by consolidation and maintenance therapy for 12 months (post-HCT excluded) in newly diagnosed patients with FLT3-ITD AML. Four patients were excluded in a modified intention-to-treat final analysis (3 not commencing therapy and 1 was FLT3-ITD negative). Rates of complete remission (CR)/CR with incomplete hematologic recovery were high in both arms (sorafenib, 78%/9%; placebo, 70%/24%). With 49.1-months median follow-up, the primary end point of event-free survival (EFS) was not improved by sorafenib (2-year EFS 47.9% vs 45.4%; hazard ratio [HR], 0.87; 95% confidence interval [CI], 0.51-1.51; P = .61). Two-year overall survival (OS) was 67% in the sorafenib arm and 58% in the placebo arm (HR, 0.76; 95% CI, 0.42-1.39). For patients who received HCT in first remission, the 2-year OS rates were 84% and 67% in the sorafenib and placebo arms, respectively (HR, 0.45; 95% CI, 0.18-1.12; P = .08). In exploratory analyses, FLT3-ITD measurable residual disease (MRD) negative status (<0.001%) after induction was associated with improved 2-year OS (83% vs 60%; HR, 0.4; 95% CI, 0.17-0.93; P = .028). In conclusion, routine use of pretransplant sorafenib plus chemotherapy in unselected patients with FLT3-ITD AML is not supported by this study.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: A.H.W. has served on advisory boards for Novartis, AstraZeneca, Astellas, Janssen, Amgen, Roche, Pfizer, AbbVie, Servier, Gilead, Bristol Myers Squibb, Shoreline, Macrogenics, and Agios; receives research funding to the Institution from Novartis, AbbVie, Servier, Janssen, BMS, Syndax, Astex, AstraZeneca, and Amgen; and serves on speaker’s bureaus for AbbVie, Novartis, BMS, Servier, and Astellas. A.H.W., A.W.R., and N.S.A. are employees of the Walter and Eliza Hall Institute (WEHI); WEHI receives milestone and royalty payments related to the development of venetoclax. Current and past employees of WEHI may be eligible for financial benefits related to these payments, and A.H.W., A.W.R., and N.S.A. receive such financial benefits. A.W.R. is listed as an inventor on a patent related to venetoclax assigned to AbbVie and Genentech. The remaining authors declare no competing financial interests.
Figures




Comment in
-
FLT(3)-ing about: the search for the best inhibitor.Blood. 2023 Dec 7;142(23):1937-1938. doi: 10.1182/blood.2023022174. Blood. 2023. PMID: 38060271 No abstract available.
References
-
- Nakao M, Yokota S, Iwai T, et al. Internal tandem duplication of the flt3 gene found in acute myeloid leukemia. Leukemia. 1996;10(12):1911–1918. - PubMed
-
- Metzeler KH, Herold T, Rothenberg-Thurley M, et al. Spectrum and prognostic relevance of driver gene mutations in acute myeloid leukemia. Blood. 2016;128(5):686–698. - PubMed
-
- Gale R, Green C, Allen C, et al. The impact of FLT3 internal tandem duplication mutant level, number, size, and interaction with NPM1 mutations in a large cohort of young adult patients with acute myeloid leukemia. Blood. 2008;111(5):2776–2784. - PubMed
-
- Perl AE, Martinelli G, Cortes JE, et al. Gilteritinib or chemotherapy for relapsed or refractory FLT3-mutated AML. N Engl J Med. 2019;381(18):1728–1740. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
