

Expedited transfer to a cardiac arrest centre for non-ST-elevation out-of-hospital cardiac arrest (ARREST): a UK prospective, multicentre, parallel, randomised clinical trial
- PMID: 37647928
- PMCID: PMC10877072
- DOI: 10.1016/S0140-6736(23)01351-X
Expedited transfer to a cardiac arrest centre for non-ST-elevation out-of-hospital cardiac arrest (ARREST): a UK prospective, multicentre, parallel, randomised clinical trial
Abstract
Background: The International Liaison Committee on Resuscitation has called for a randomised trial of delivery to a cardiac arrest centre. We aimed to assess whether expedited delivery to a cardiac arrest centre compared with current standard of care following resuscitated cardiac arrest reduces deaths.
Methods: ARREST is a prospective, parallel, multicentre, open-label, randomised superiority trial. Patients (aged ≥18 years) with return of spontaneous circulation following out-of-hospital cardiac arrest without ST elevation were randomly assigned (1:1) at the scene of their cardiac arrest by London Ambulance Service staff using a secure online randomisation system to expedited delivery to the cardiac catheter laboratory at one of seven cardiac arrest centres or standard of care with delivery to the geographically closest emergency department at one of 32 hospitals in London, UK. Masking of the ambulance staff who delivered the interventions and those reporting treatment outcomes in hospital was not possible. The primary outcome was all-cause mortality at 30 days, analysed in the intention-to-treat (ITT) population excluding those with unknown mortality status. Safety outcomes were analysed in the ITT population. The trial was prospectively registered with the International Standard Randomised Controlled Trials Registry, 96585404.
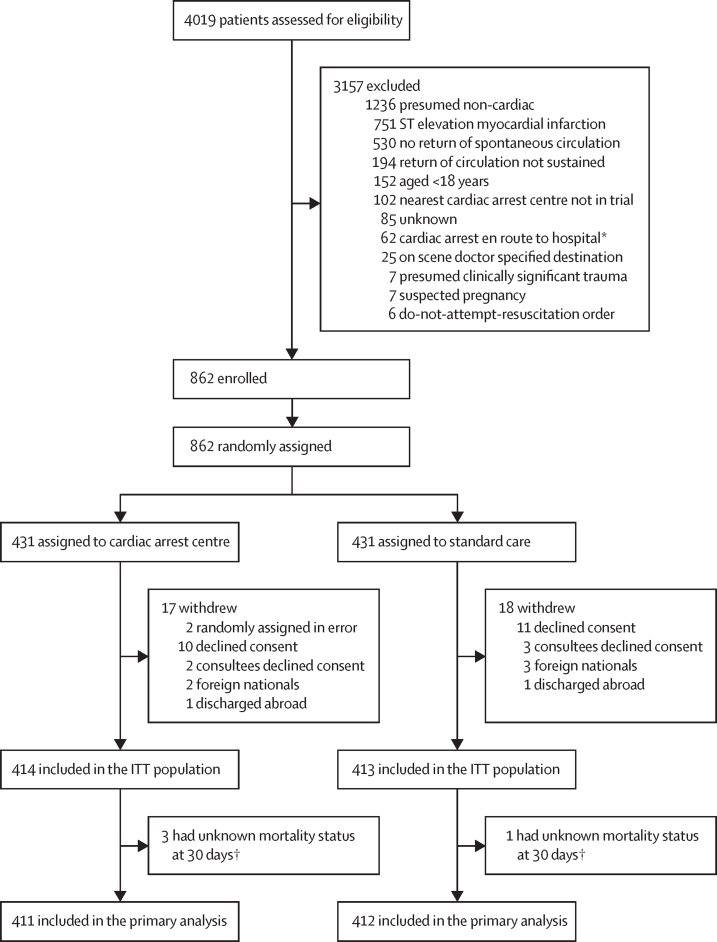
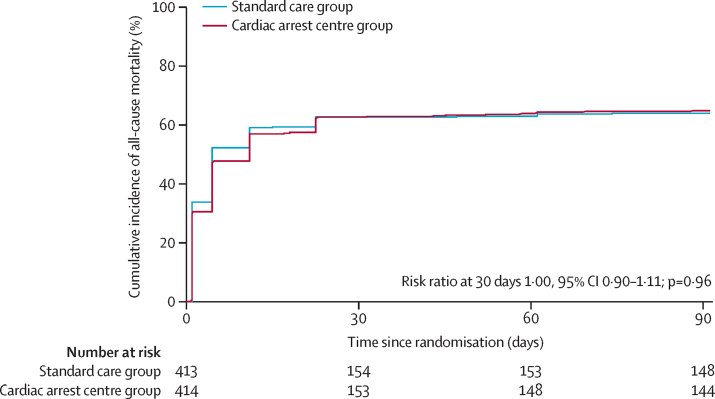
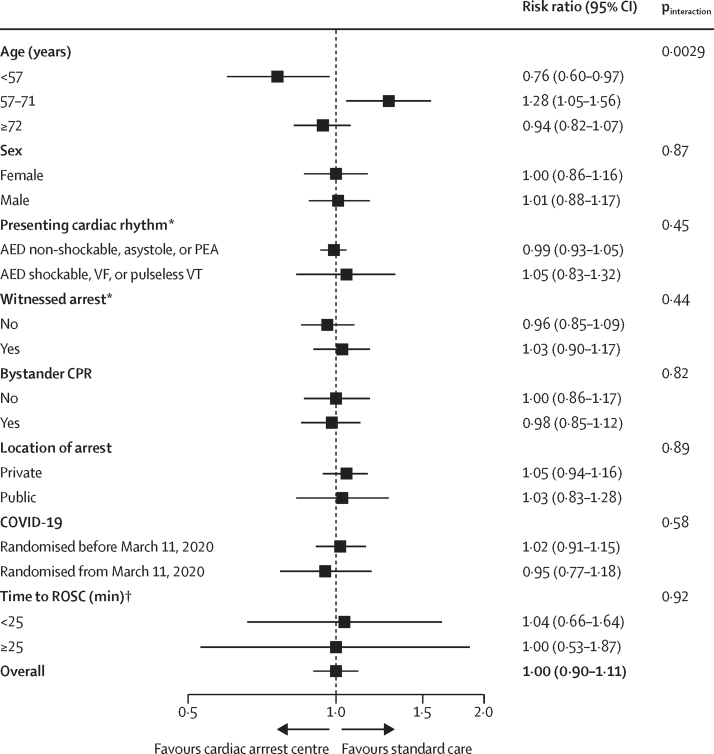
Findings: Between Jan 15, 2018, and Dec 1, 2022, 862 patients were enrolled, of whom 431 (50%) were randomly assigned to a cardiac arrest centre and 431 (50%) to standard care. 20 participants withdrew from the cardiac arrest centre group and 19 from the standard care group, due to lack of consent or unknown mortality status, leaving 411 participants in the cardiac arrest centre group and 412 in the standard care group for the primary analysis. Of 822 participants for whom data were available, 560 (68%) were male and 262 (32%) were female. The primary endpoint of 30-day mortality occurred in 258 (63%) of 411 participants in the cardiac arrest centre group and in 258 (63%) of 412 in the standard care group (unadjusted risk ratio for survival 1·00, 95% CI 0·90-1·11; p=0·96). Eight (2%) of 414 patients in the cardiac arrest centre group and three (1%) of 413 in the standard care group had serious adverse events, none of which were deemed related to the trial intervention.
Interpretation: In adult patients without ST elevation, transfer to a cardiac arrest centre following resuscitated cardiac arrest in the community did not reduce deaths.
Funding: British Heart Foundation.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
References
-
- Perkins GD, Cooke MW. Variability in cardiac arrest survival: the NHS Ambulance Service Quality Indicators. Emerg Med J. 2012;29:3–5. - PubMed
-
- Perkins GD, Jacobs IG, Nadkarni VM, et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update of the Utstein Resuscitation Registry templates for out-of-hospital cardiac arrest: a statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Resuscitation. 2015;96:328–340. - PubMed
-
- Jacobs AK, Ali MJ, Best PJ, et al. Systems of care for ST-segment-elevation myocardial infarction: a policy statement from the American Heart Association. Circulation. 2021;144:e310–e327. - PubMed
-
- Nichol G, Aufderheide TP, Eigel B, et al. Regional systems of care for out-of-hospital cardiac arrest: a policy statement from the American Heart Association. Circulation. 2010;121:709–729. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
