

Scapula-Focused Exercises With or Without Biofeedback and Corticospinal Excitability in Recreational Overhead Athletes With Shoulder Impingement
- PMID: 37648216
- PMCID: PMC11220774
- DOI: 10.4085/1062-6050-0066.23
Scapula-Focused Exercises With or Without Biofeedback and Corticospinal Excitability in Recreational Overhead Athletes With Shoulder Impingement
Abstract
Context: Individuals with shoulder impingement syndrome (SIS) exhibit changes in corticospinal excitability, scapular kinematics, and scapular muscle-activation patterns. To restore the scapular kinematics and muscle-activation patterns in individuals with SIS, treatment protocols usually include scapula-focused exercises, such as scapular-orientation and strength training.
Objective: To investigate whether scapular-orientation and strength training can reverse the altered corticospinal excitability of recreational overhead athletes with SIS.
Design: Randomized controlled clinical trial.
Setting: University laboratory.
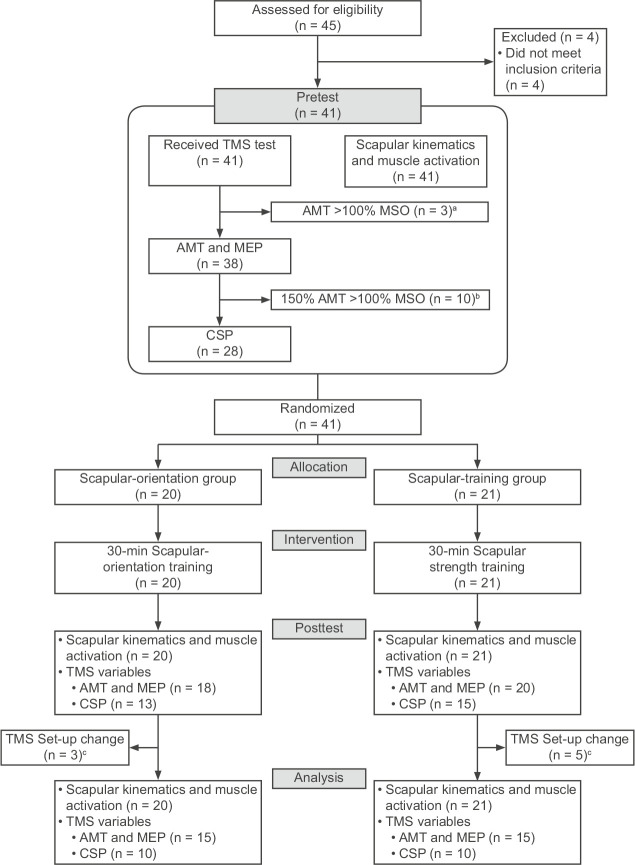
Patients or other participants: Forty-one recreational overhead athletes with SIS: 20 in the scapular-orientation group (age = 26.45 ± 4.13 years, height = 171.85 ± 7.88 cm, mass = 66.70 ± 10.68 kg) and 21 in the strengthening group (age = 26.43 ± 5.55 years, height = 171.62 ± 5.87 cm, mass = 68.67 ± 10.18 kg).
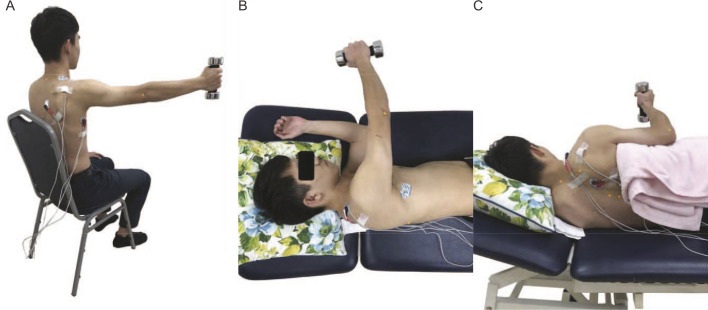
Intervention(s): Both groups performed a 30-minute training protocol consisting of 3 exercises to strengthen the lower trapezius (LT) and serratus anterior muscles without overactivating the upper trapezius muscles. Participants in the scapular-orientation group were instructed to consciously activate their scapular muscles with electromyographic biofeedback and cues, whereas the strengthening group did not receive biofeedback or cues for scapular motion.
Main outcome measure(s): Corticospinal excitability was assessed using transcranial magnetic stimulation. Scapular kinematics and muscle activation during arm elevation were also measured.
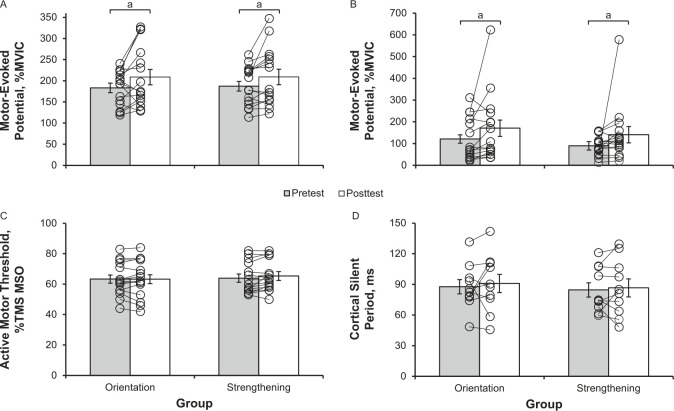
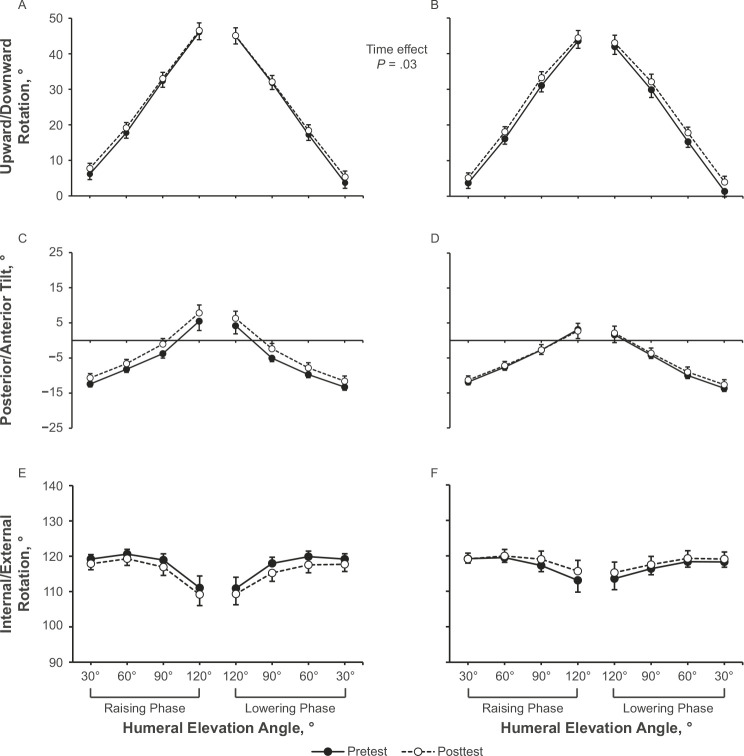
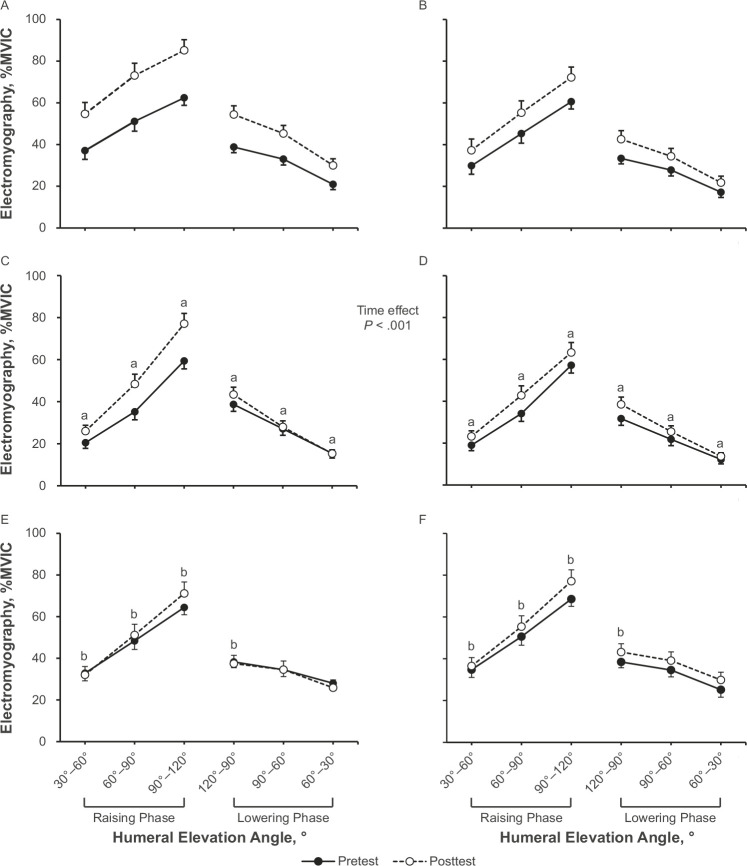
Results: After training, both groups demonstrated an increase in motor-evoked potentials in the LT (P = .004) and increases in scapular upward rotation (P = .03), LT activation (P < .001), and serratus anterior activation (P < .001) during arm elevation. Moreover, the scapular-orientation group showed higher LT activation levels during arm elevation after training than the strengthening group (P = .03).
Conclusions: With or without biofeedback and cues, scapula-focused exercises improved scapular control and increased corticospinal excitability. Adding biofeedback and cues for scapular control during exercise helped facilitate greater LT activation, so feedback and cues are recommended during scapula-focused training.
Keywords: scapular dyskinesis; scapular-orientation exercise; strength training; transcranial magnetic stimulation.
© by the National Athletic Trainers' Association, Inc.
Figures
Similar articles
-
Single-Session Video and Electromyography Feedback in Overhead Athletes With Scapular Dyskinesis and Impingement Syndrome.J Athl Train. 2020 Mar;55(3):265-273. doi: 10.4085/1062-6050-490-18. Epub 2019 Dec 26. J Athl Train. 2020. PMID: 31876455 Free PMC article. Clinical Trial.
-
Progressive conscious control of scapular orientation with video feedback has improvement in muscle balance ratio in patients with scapular dyskinesis: a randomized controlled trial.J Shoulder Elbow Surg. 2018 Aug;27(8):1407-1414. doi: 10.1016/j.jse.2018.04.006. Epub 2018 Jun 6. J Shoulder Elbow Surg. 2018. PMID: 29886062 Clinical Trial.
-
Effects of Kinesiology Taping on Scapular Reposition Accuracy, Kinematics, and Muscle Activity in Athletes With Shoulder Impingement Syndrome: A Randomized Controlled Study.J Sport Rehabil. 2018 Nov 1;27(6):560-569. doi: 10.1123/jsr.2017-0043. Epub 2018 Oct 15. J Sport Rehabil. 2018. PMID: 29364027 Clinical Trial.
-
Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement.Phys Ther. 2000 Mar;80(3):276-91. Phys Ther. 2000. PMID: 10696154 Review.
-
Scapular dyskinesis and overhead athletes: A systematic review of electromyography studies.J Bodyw Mov Ther. 2024 Jul;39:606-614. doi: 10.1016/j.jbmt.2024.03.014. Epub 2024 Mar 16. J Bodyw Mov Ther. 2024. PMID: 38876694
Cited by
-
Therapeutic Exercise Prescription for Overhead Athletes with Shoulder Impingement Syndrome: A Systematic Review and CERT Analysis.J Clin Med. 2025 Feb 28;14(5):1657. doi: 10.3390/jcm14051657. J Clin Med. 2025. PMID: 40095639 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
