

Ablation to Reduce Atrial Fibrillation Burden and Improve Outcomes: JACC Review Topic of the Week
- PMID: 37648353
- PMCID: PMC11103629
- DOI: 10.1016/j.jacc.2023.06.029
Ablation to Reduce Atrial Fibrillation Burden and Improve Outcomes: JACC Review Topic of the Week
Abstract
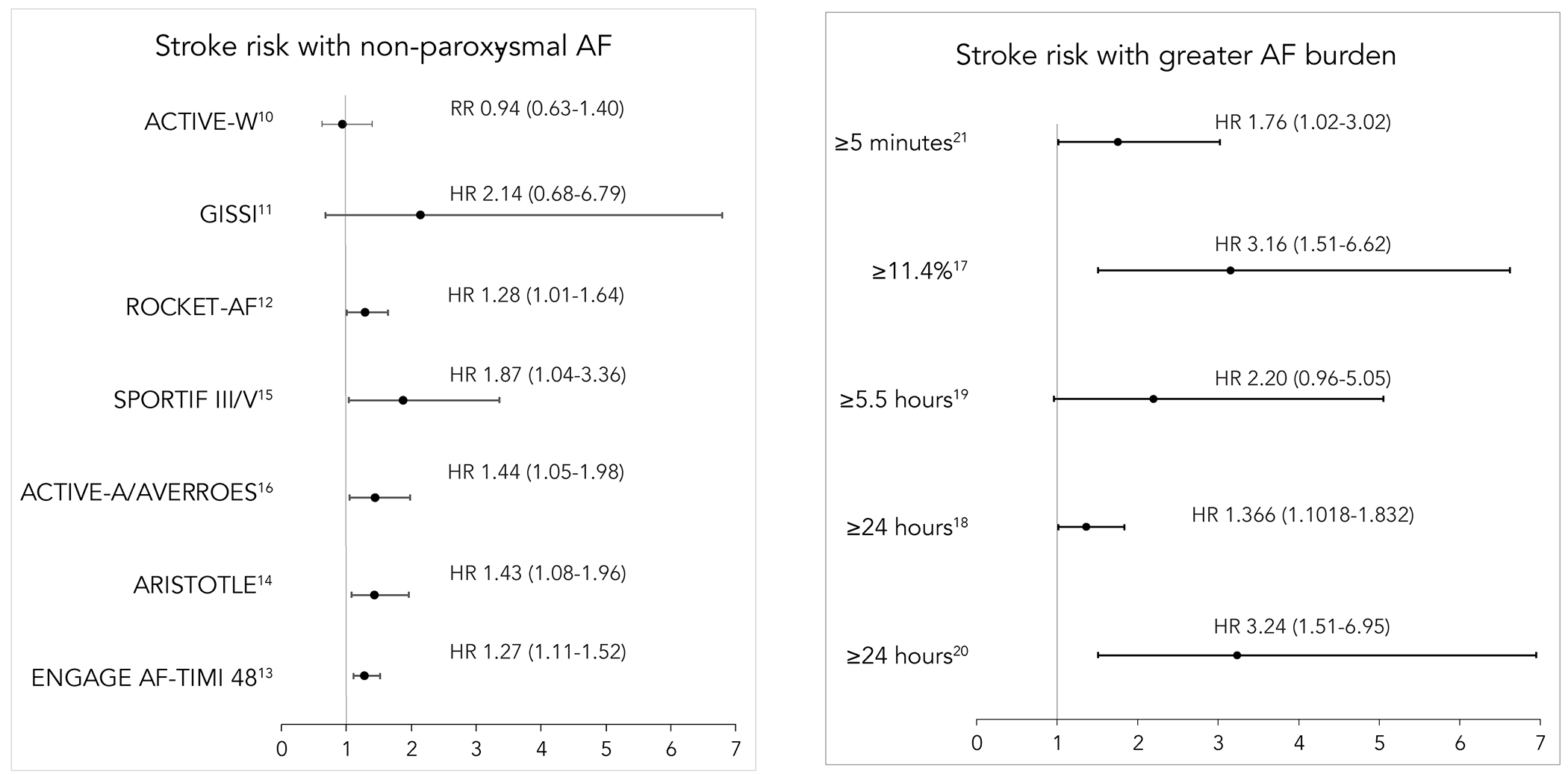
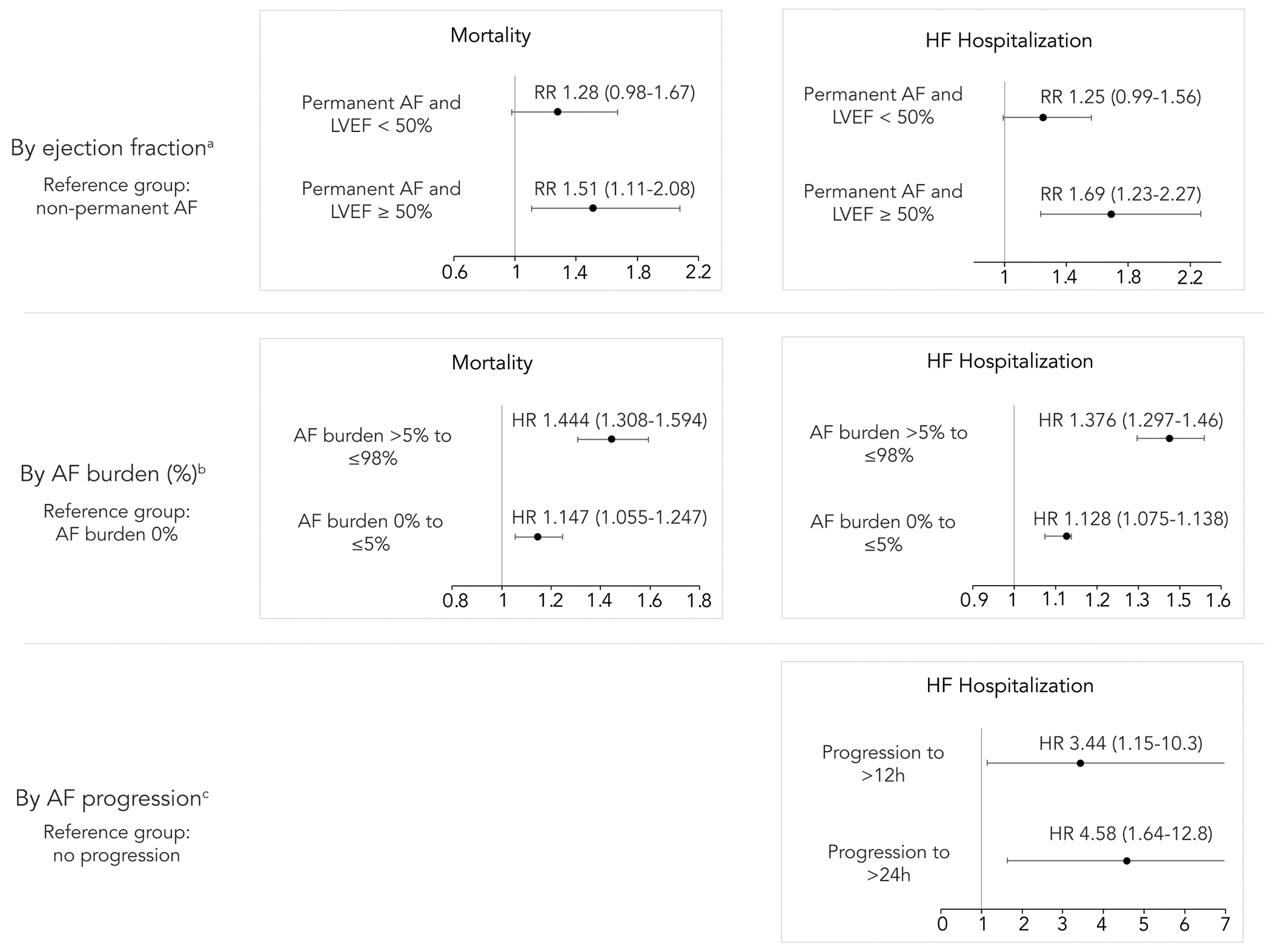
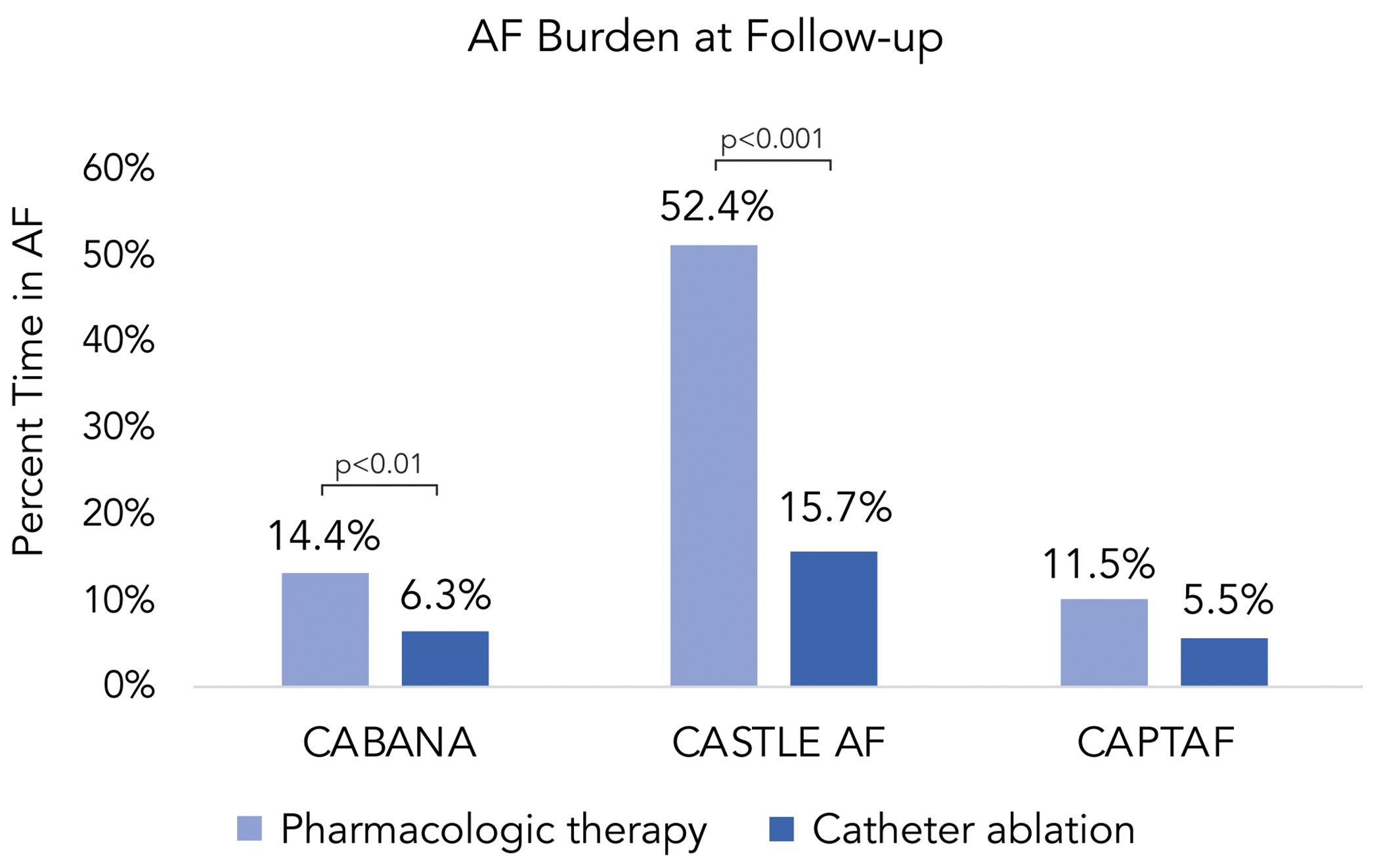
Atrial fibrillation is the most common atrial arrhythmia and accounts for a significant burden of cardiovascular disease globally. With advances in implanted and wearable cardiac monitoring technology, it is now possible to readily and accurately quantify an individual's time spent in atrial fibrillation. This review summarizes the relationship between atrial fibrillation burden and adverse cardiovascular and cerebrovascular outcomes and discusses the role of catheter ablation to mitigate the morbidity and mortality associated with greater burden of atrial fibrillation.
Keywords: catheter ablation; heart failure; mortality; stroke.
Copyright © 2023 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Andrade has received grants and personal fees from Medtronic; has received grants from Baylis; and has received personal fees from Biosense-Webster. Dr Wood has received honoraria for speaking/consulting from Milestone Pharmaceuticals. Dr Piccini is supported by R01AG074185 from the National Institutes of Aging; has received grants for clinical research from Abbott, the American Heart Association, the Association for the Advancement of Medical Instrumentation, Bayer, Boston Scientific, iRhythm, and Philips; and has served as a consultant to Abbott, AbbVie, ARCA Biopharma, Bayer, Boston Scientific, Bristol Myers Squibb (Myokardia), Element Science, Itamar Medical, LivaNova, Medtronic, Milestone, ElectroPhysiology Frontiers, ReCor, Sanofi, Philips, and Up-to-Date. Dr Schwennesen has reported that she has no relationships relevant to the contents of this paper to disclose.
Figures


References
-
- January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation. J Am Coll Cardiol. 2014;64:e1–e76. - PubMed
-
- Andrade JG, Yao RRJ, Deyell MW, et al. Clinical assessment of AF pattern is poorly correlated with AF burden and post ablation outcomes: A CIRCA-DOSE sub-study. J Electrocardiol. 2020;60:159–164. - PubMed
-
- Charitos EI, Pürerfellner H, Glotzer TV, Ziegler PD. Clinical Classifications of Atrial Fibrillation Poorly Reflect Its Temporal Persistence. J Am Coll Cardiol. 2014;63:2840–2848. - PubMed
-
- Flaker GC, Belew K, Beckman K, et al. Asymptomatic atrial fibrillation: Demographic features and prognostic information from the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study. Am Heart J. 2005;149:657–663. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
