

Effect of preoperative oral rehydration before cesarean section on ultrasound assessment of gastric volume and intraoperative hemodynamic changes: a randomized controlled trial
- PMID: 37648966
- PMCID: PMC10466736
- DOI: 10.1186/s12871-023-02250-6
Effect of preoperative oral rehydration before cesarean section on ultrasound assessment of gastric volume and intraoperative hemodynamic changes: a randomized controlled trial
Abstract
Background: Cesarean section often requires an urgent transfusion load due to decreased blood pressure after spinal anesthesia. This prospective randomized study aimed to investigate whether a preoperative oral rehydration solution (ORS) stabilized perioperative circulatory dynamics.
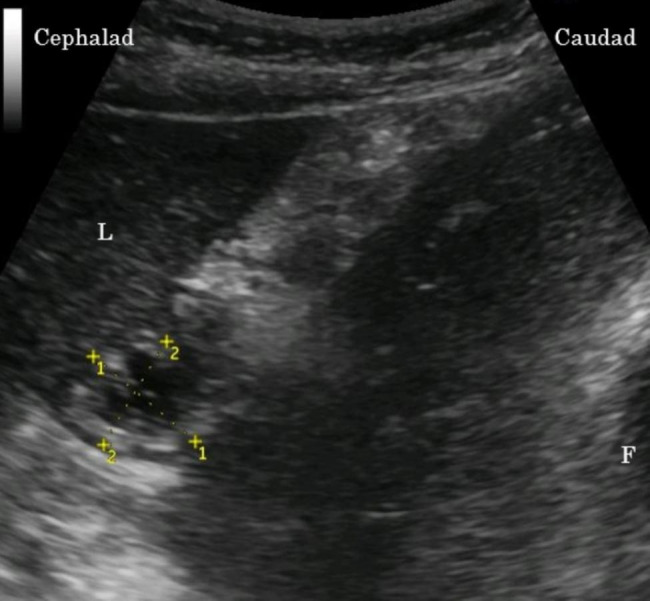
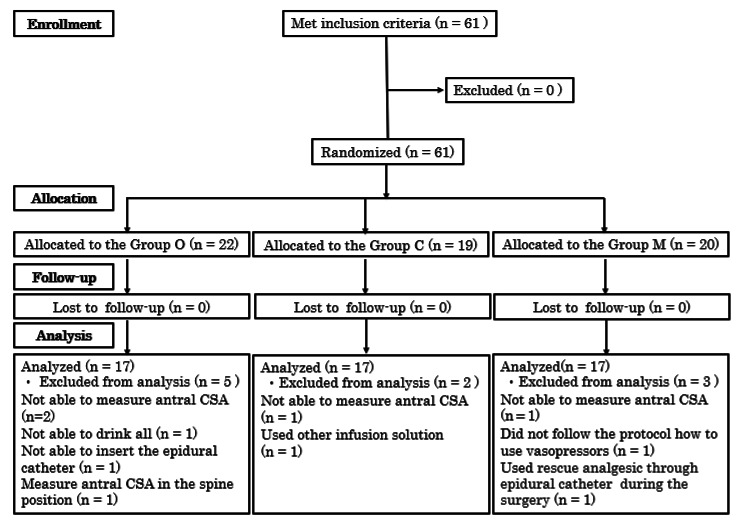
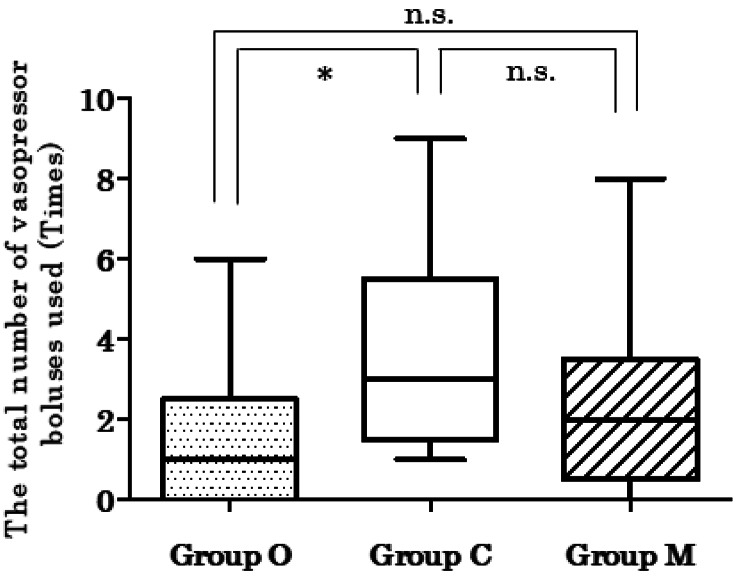
Methods: Sixty-three parturients scheduled for cesarean section under combined spinal epidural anesthesia (CSEA) were randomly allocated to one of three groups: Group O received 500 mL ORS before bedtime and 500 mL 2 h before CSEA; Group M received mineral water instead of ORS; and Group C had no fluid intake (controls). After entering the operating room, stomach size was measured using ultrasound. Blood samples were obtained, and CSEA was induced. Vasopressors were administered when systolic blood pressure was < 90 mmHg or decreased by > 20%. As a vasopressor, phenylephrine (0.1 mg) was administered at ≥ 60 beats/min heart rate or ephedrine (5 mg) at < 60 beats/min heart rate. The primary outcome was the total number of vasopressor boluses administered. Secondary outcomes were the cross-sectional area of the stomach antrum, maternal plasma glucose levels, serum sodium levels, total intravenous fluid, bleeding volume, urine volume, operative time, and cord blood gas values after delivery.
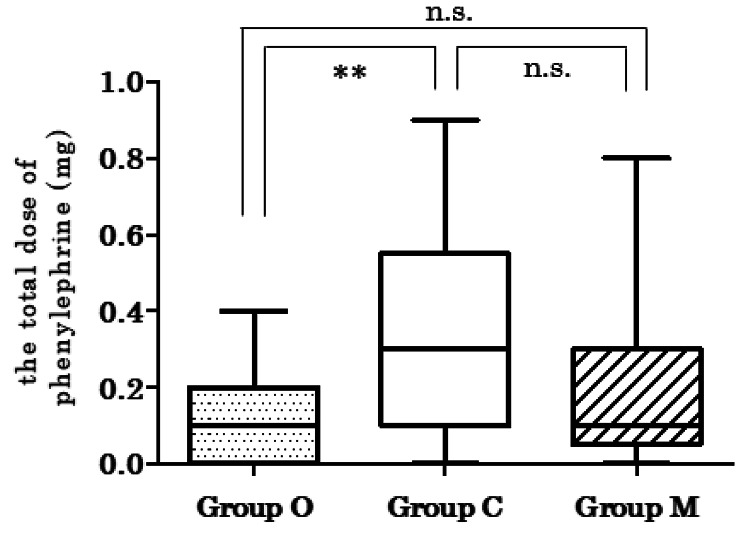
Results: The total number of vasopressor boluses was lower in Group O than in Group C (P < 0.05). Group O had lower total dose of phenylephrine than Group C (P < 0.05). There were no significant differences between Group M and other groups. No differences were detected regarding secondary outcomes.
Conclusions: In women scheduled for cesarean section, preoperative ORS stabilized perioperative circulatory dynamics. Neither ORS nor mineral water consumption increased the stomach content volume.
Trial registration: This trial is registered in the University Hospital Medical Information Network Clinical Trials Registry (UMIN000019825: Date of registration 17/11/2015).
Keywords: Cesarean section; Gastric volume; Oral rehydration therapy; Preoperative fasting; Preoperative management.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Evaluating an advanced double intravenous vasopressor automated system to treat hypotension during spinal anesthesia for cesarean delivery: a randomized controlled trial.BMC Anesthesiol. 2023 Jan 26;23(1):33. doi: 10.1186/s12871-023-01992-7. BMC Anesthesiol. 2023. PMID: 36703120 Free PMC article. Clinical Trial.
-
Norepinephrine versus phenylephrine infusion for preventing postspinal hypotension during cesarean section for twin pregnancy: a double-blinded randomized controlled clinical trial.BMC Anesthesiol. 2022 Jan 8;22(1):17. doi: 10.1186/s12871-022-01562-3. BMC Anesthesiol. 2022. PMID: 34998371 Free PMC article. Clinical Trial.
-
Maternal cardiac output changes after crystalloid or colloid coload following spinal anesthesia for elective cesarean delivery: a randomized controlled trial.Anesth Analg. 2011 Oct;113(4):803-10. doi: 10.1213/ANE.0b013e31822c0f08. Epub 2011 Sep 2. Anesth Analg. 2011. PMID: 21890886 Clinical Trial.
-
Phenylephrine vs ephedrine in cesarean delivery under spinal anesthesia: A systematic literature review and meta-analysis.Int J Surg. 2018 Dec;60:48-59. doi: 10.1016/j.ijsu.2018.10.039. Epub 2018 Oct 31. Int J Surg. 2018. PMID: 30389535
-
Efficacy and safety of norepinephrine versus phenylephrine for the management of maternal hypotension during cesarean delivery with spinal anesthesia: A systematic review and meta-analysis.Medicine (Baltimore). 2019 Feb;98(5):e14331. doi: 10.1097/MD.0000000000014331. Medicine (Baltimore). 2019. PMID: 30702617 Free PMC article.
Cited by
-
Gastric emptying in pregnancy and its clinical implications: a narrative review.Br J Anaesth. 2025 Jan;134(1):124-167. doi: 10.1016/j.bja.2024.09.005. Epub 2024 Oct 22. Br J Anaesth. 2025. PMID: 39443186 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Associated data
- Actions
LinkOut - more resources
Full Text Sources
Medical
Research Materials
