

Updating mortality risk estimation in intensive care units from high-dimensional electronic health records with incomplete data
- PMID: 37648995
- PMCID: PMC10466694
- DOI: 10.1186/s12911-023-02264-7
Updating mortality risk estimation in intensive care units from high-dimensional electronic health records with incomplete data
Abstract
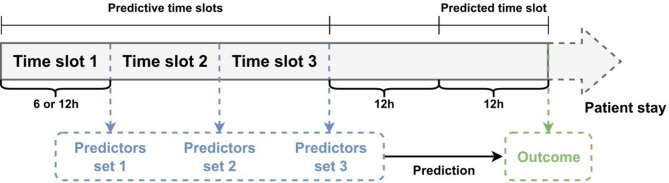
Background: The risk of mortality in intensive care units (ICUs) is currently addressed by the implementation of scores using admission data. Their performances are satisfactory when complications occur early after admission; however, they may become irrelevant in the case of long hospital stays. In this study, we developed predictive models of short-term mortality in the ICU from longitudinal data.
Methods: Using data collected throughout patients' stays of at least 48 h from the MIMIC-III database, several statistical learning approaches were compared, including deep neural networks and penalized regression. Missing data were handled using complete-case analysis or multiple imputation.
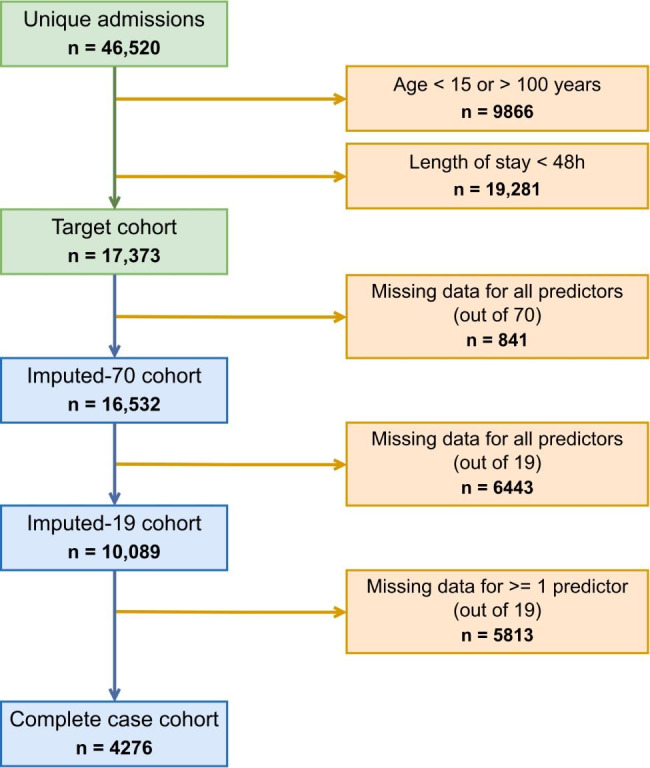
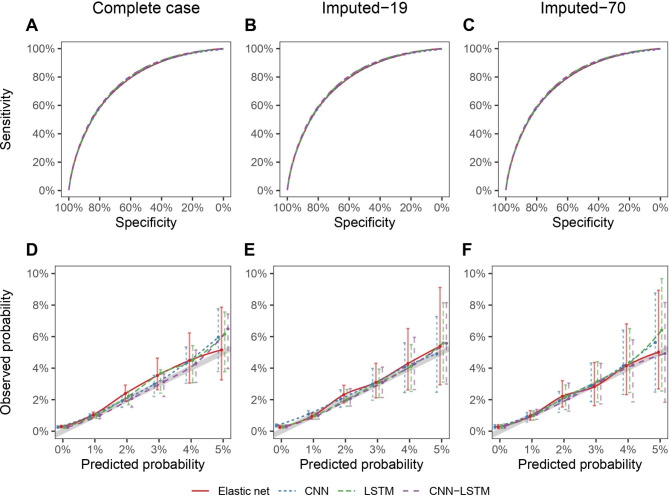
Results: Complete-case analyses from 19 predictors showed good discrimination (AUC > 0.77 for several approaches) to predict death between 12 and 24 h onward, yet excluded 75% of patients from the initial target cohort, as data was missing for some of the predictors. Multiple imputation allowed us to include 70 predictors and keep 95% of patients, with similar performances.
Conclusion: This proof-of-concept study supports that automated analysis of electronic health records can be of great interest throughout patients' stays as a surveillance tool. Although this framework relies on a large set of predictors, it is robust to data imputation and may be effective early after admission, when data are still scarce.
Keywords: Clinical decision support systems; Electronic health records; Machine learning; Multiple imputation; Neural network.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22:707–10. doi: 10.1007/BF01709751. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
