

Variations in the prevalence of caesarean section deliveries in India between 2016 and 2021 - an analysis of Tamil Nadu and Chhattisgarh
- PMID: 37649006
- PMCID: PMC10466745
- DOI: 10.1186/s12884-023-05928-4
Variations in the prevalence of caesarean section deliveries in India between 2016 and 2021 - an analysis of Tamil Nadu and Chhattisgarh
Erratum in
-
Correction: Variations in the prevalence of caesarean section deliveries in India between 2016 and 2021 - an analysis of Tamil Nadu and Chhattisgarh.BMC Pregnancy Childbirth. 2023 Sep 26;23(1):693. doi: 10.1186/s12884-023-06020-7. BMC Pregnancy Childbirth. 2023. PMID: 37752430 Free PMC article. No abstract available.
Abstract
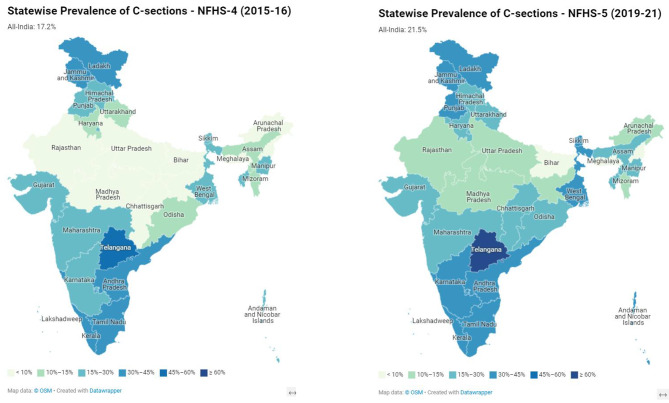
Background: The prevalence of C-sections in India increased from 17.2% to 2006 to 21.5% in 2021. This study examines the variations in C-section prevalence and the factors correlating to these variations in Tamil Nadu (TN) and Chhattisgarh (CG).
Methods: Delivery by C-section as the outcome variable and several demographic, socio-economic, and clinical variables were considered as explanatory variables to draw inferences from unit-level data from the National Family Health Survey (NFHS-4; 2015-16 and NFHS-5; 2019-21). Descriptive statistics, bivariate percentage distribution, Pearson's Chi-square test, and multivariate binary logistic regression models were employed. The Slope Index of Inequality (SII) and the Concentration Index (CIX) were used to analyse absolute and relative inequality in C-section rates across wealth quintiles in public- and private-sector institutions.
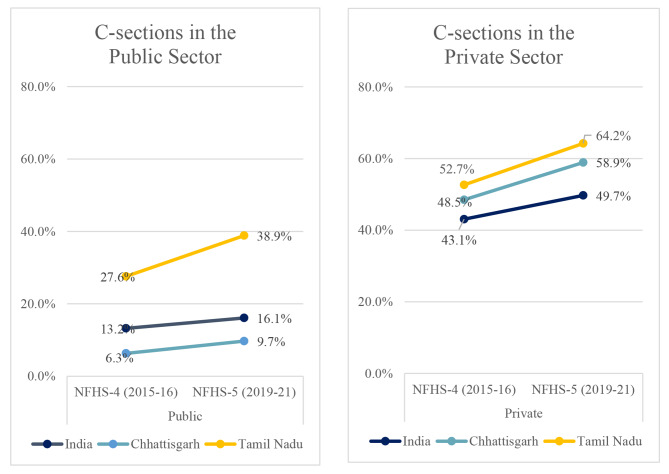
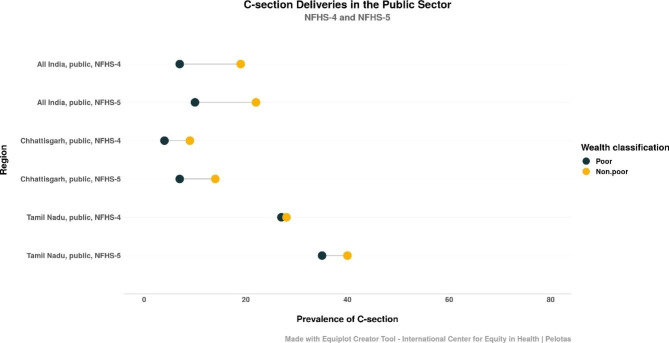
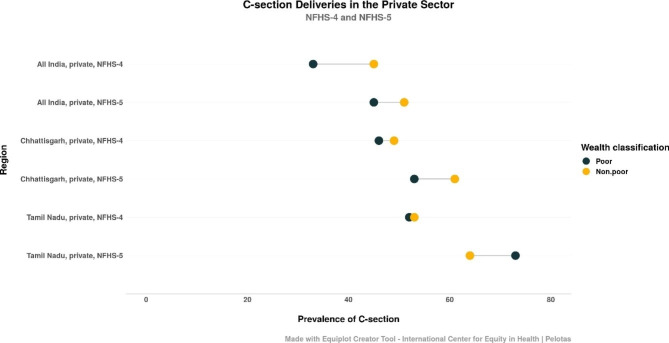
Results: The prevalence of C-sections increased across India, TN and CG despite a decrease in pregnancy complications among the study participants. The odds of caesarean deliveries among overweight women were twice (OR = 2.11; 95% CI 1.95-2.29; NFHS-5) those for underweight women. Women aged 35-49 were also twice (OR = 2.10; 95% CI 1.92-2.29; NFHS-5) as likely as those aged 15-24 to have C-sections. In India, women delivering in private health facilities had nearly four times higher odds (OR = 3.90; 95% CI 3.74-4.06; NFHS-5) of having a C-section; in CG, the odds were nearly ten-fold (OR = 9.57; 95% CI:7.51,12.20; NFHS-5); and in TN, nearly three-fold (OR = 2.65; 95% CI-2.27-3.10; NFHS-5) compared to those delivering in public facilities. In public facilities, absolute inequality by wealth quintile in C-section prevalence across India and in CG increased in the five years until 2021, indicating that the rich increasingly delivered via C-sections. In private facilities, the gap in C-section prevalence between the poor (the bottom two quintiles) and the non-poor narrowed across India. In TN, the pattern was inverted in 2021, with an alarming 73% of the poor delivering via C-sections compared to 64% of those classified as non-poor.
Conclusion: The type of health facility (public or private) had the most impact on whether delivery was by C-section. In India and CG, the rich are more likely to have C-sections, both in the private and in the public sector. In TN, a state with good health indicators overall, the poor are surprisingly more likely to have C-sections in the private sector. While the reasons for this inversion are not immediately evident, the implications are worrisome and pose public health policy challenges.
Keywords: C-section delivery; Caesarean section; India; Inequality; NFHS-5; Private Sector.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Geographical variability and factors associated with caesarean section delivery in India: a comparative assessment of Bihar and Tamil Nadu.BMC Public Health. 2021 Sep 21;21(1):1715. doi: 10.1186/s12889-021-11750-4. BMC Public Health. 2021. PMID: 34548059 Free PMC article.
-
Assessment of Variation in Cesarean Delivery Rates Between Public and Private Health Facilities in India From 2005 to 2016.JAMA Netw Open. 2020 Aug 3;3(8):e2015022. doi: 10.1001/jamanetworkopen.2020.15022. JAMA Netw Open. 2020. PMID: 32857148 Free PMC article.
-
High prevalence of cesarean section births in private sector health facilities- analysis of district level household survey-4 (DLHS-4) of India.BMC Public Health. 2018 May 10;18(1):613. doi: 10.1186/s12889-018-5533-3. BMC Public Health. 2018. PMID: 29747609 Free PMC article.
-
Are cesarean deliveries equitable in India: assessment using benefit incidence analysis.BMC Health Serv Res. 2022 May 18;22(1):670. doi: 10.1186/s12913-022-07984-6. BMC Health Serv Res. 2022. PMID: 35585584 Free PMC article.
-
A Comparative Study of National Family Health Survey-4 and National Family Health Survey-5 of Nutritional Indicators in Chhattisgarh.Cureus. 2024 Mar 4;16(3):e55524. doi: 10.7759/cureus.55524. eCollection 2024 Mar. Cureus. 2024. PMID: 38576647 Free PMC article. Review.
Cited by
-
State-wise variation and inequalities in caesarean delivery rates in India: analysis of the National Family Health Survey-5 (2019-2021) data.Lancet Reg Health Southeast Asia. 2024 Dec 3;32:100512. doi: 10.1016/j.lansea.2024.100512. eCollection 2025 Jan. Lancet Reg Health Southeast Asia. 2024. PMID: 39717057 Free PMC article.
-
Anesthetic Challenges and Management of Obstetric Emergencies in a Secondary Care Hospital in a Remote Mining Area: A Case Series.Cureus. 2024 Sep 4;16(9):e68675. doi: 10.7759/cureus.68675. eCollection 2024 Sep. Cureus. 2024. PMID: 39371864 Free PMC article.
-
Determinants of cesarean section in urban areas of Bangladesh: Insights from the Bangladesh Demographic and Health Survey-2022.Womens Health (Lond). 2025 Jan-Dec;21:17455057251356806. doi: 10.1177/17455057251356806. Epub 2025 Aug 11. Womens Health (Lond). 2025. PMID: 40785446 Free PMC article.
-
Correction: Variations in the prevalence of caesarean section deliveries in India between 2016 and 2021 - an analysis of Tamil Nadu and Chhattisgarh.BMC Pregnancy Childbirth. 2023 Sep 26;23(1):693. doi: 10.1186/s12884-023-06020-7. BMC Pregnancy Childbirth. 2023. PMID: 37752430 Free PMC article. No abstract available.
-
Comparison of Three Techniques for Skin Closure in Caesarean Delivery (Absorbable Subcuticular Sutures, Non-absorbable Nylon Sutures, Surgical Staplers): A Randomized Controlled Trial.J Obstet Gynaecol India. 2025 Apr;75(Suppl 1):348-354. doi: 10.1007/s13224-024-01999-1. Epub 2024 Jun 13. J Obstet Gynaecol India. 2025. PMID: 40390946
References
-
- Gregory KD, Jackson S, Korst L, Fridman M. Cesarean versus vaginal delivery: whose risks? Whose benefits? Am J Perinatol. 2012;29. - PubMed
-
- Sandall J, Tribe RM, Avery L, Mola G, Visser GH, Homer CS et al. Short-term and long-term effects of caesarean section on the health of women and children. The Lancet. 2018;392(10155):1349–57. Available from: http://www.thelancet.com/article/S0140673618319305/fulltext. - PubMed
-
- Surana M, Dongre A. Too much care: private healthcare sector and caesarean sections in India. Econ Polit Wkly. 2020;55(35).
-
- Matevosyan NR. The overuse of Cesarean Section: Medical, Legal, Research, and economical pitfalls. J Knowl Econ. 2015;6(4):1090–103. doi: 10.1007/s13132-013-0178-z. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
