

Diagnostic dilemma in a patient with history of medullary thyroid carcinoma and abnormal serum liver enzymes; a case report with six years follow up
- PMID: 37649029
- PMCID: PMC10466678
- DOI: 10.1186/s12902-023-01439-7
Diagnostic dilemma in a patient with history of medullary thyroid carcinoma and abnormal serum liver enzymes; a case report with six years follow up
Abstract
Background: Medullary thyroid carcinoma (MTC) is a neuroendocrine tumor that originates from parafollicular C-cells. Calcitonin (Ctn) and carcinoembryonic antigen (CEA) are useful biomarkers for monitoring MTC cases.
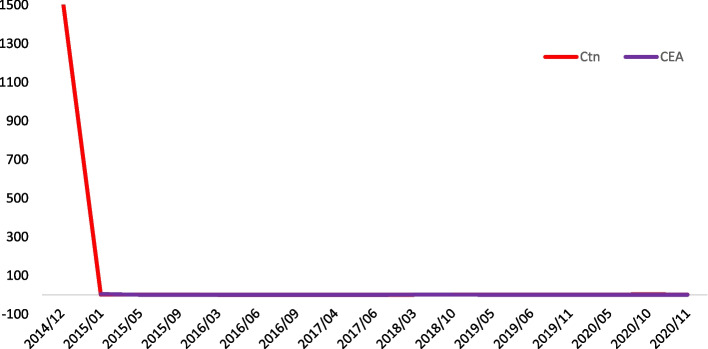
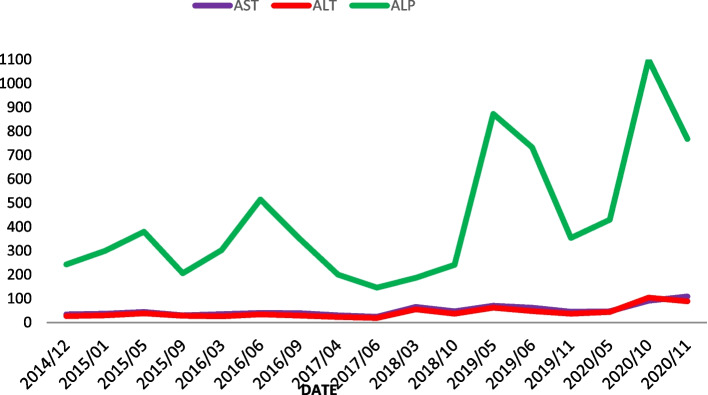
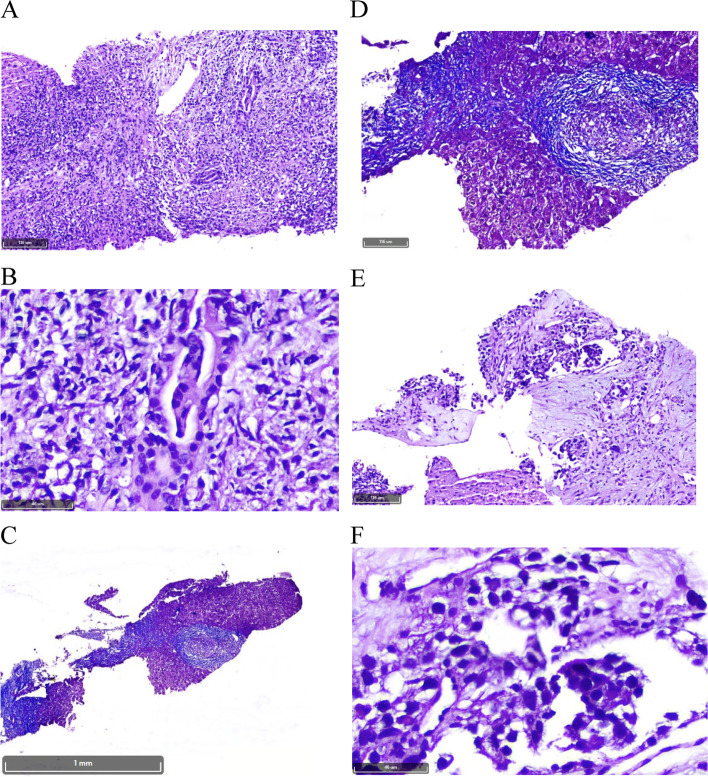
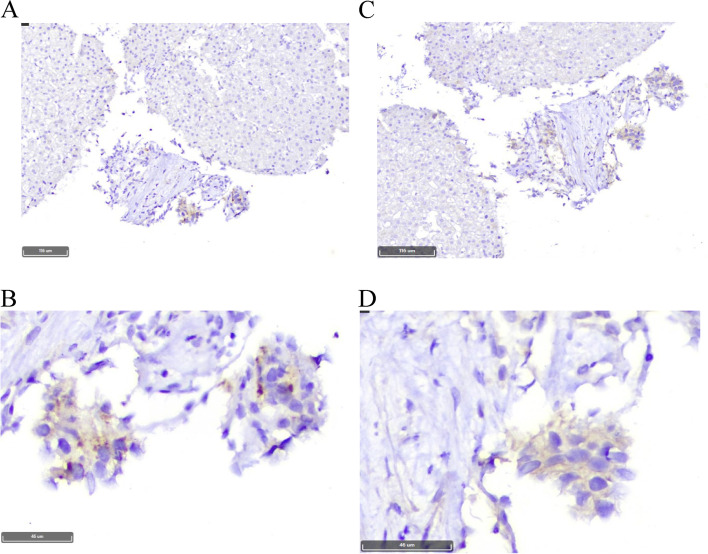
Case presentation: Here, we describe a 48-year-old woman, who presented in 2014 with bilateral thyroid nodules. Report of fine needle aspiration was suspicious for MTC; initial laboratory evaluation showed serum Ctn level of 1567 pg/mL. After excluding type 2 multiple endocrine neoplasia syndrome clinically, total thyroidectomy and neck lymph node dissection were performed. The final histopathological diagnosis was right lobe MTC with neither vascular invasion nor lymph node involvement. On regular follow-up visits, Ctn and CEA levels have been undetectable, and repeated cervical ultrasonographic exams were unremarkable from 2014 to 2021. As liver enzymes became elevated in 2016, the patient was further evaluated by a gastroenterologist. Abdominopelvic ultrasonography revealed a coarse echo pattern of the liver parenchyma with normal bile ducts. A liver fibroscan showed a low fibrosis score (7kPa). The patient was recommended to use ursodeoxycholic acid. According to the progressive rise of liver enzymes with a cholestatic pattern in October 2020, a liver biopsy was performed that showed tiny nests of neuroendocrine-like cells with a background of primary biliary cholangitis (PBC). Immunohistochemical stainings were positive for chromogranin A (CgA), and synaptophysin and negative for Ctn, CEA, and thyroglobulin. Further imaging investigations did not reveal any site of a neuroendocrine tumor in the body. Considering normal physical exam, imaging findings, as well as normal serum levels of Ctn, CEA, CgA, and procalcitonin, the patient was managed as a PBC.
Conclusion: In follow-up of a patient with MTC, we reported progressively increased liver enzymes with a cholestatic pattern. Liver biopsy revealed nests of neuroendocrine-like cells with a background of PBC, the findings that might suggest acquiring neuroendocrine phenotype by proliferating cholangiocytes.
Keywords: Case report; Histopathology; Medullary thyroid carcinoma; Neuroendocrine tumor; Primary biliary cholangitis.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Multiple Endocrine Neoplasia Type 2B Associated Mixed Medullary and Follicular Thyroid Carcinoma in A Chinese Patient with RET M918T Germline Mutation.Endocr Metab Immune Disord Drug Targets. 2021;21(3):554-560. doi: 10.2174/1871530320666200713092633. Endocr Metab Immune Disord Drug Targets. 2021. PMID: 32660411
-
Beyond the Recommendations of the Clinical Guidelines for Medullary Thyroid Cancer - A Case Report.Rev Med Chil. 2023 Jul;151(7):947-952. doi: 10.4067/s0034-98872023000700947. Rev Med Chil. 2023. PMID: 39093185
-
Management of thyroid cancer: United Kingdom National Multidisciplinary Guidelines.J Laryngol Otol. 2016 May;130(S2):S150-S160. doi: 10.1017/S0022215116000578. J Laryngol Otol. 2016. PMID: 27841128 Free PMC article.
-
Long-Term Follow-up in Medullary Thyroid Carcinoma.Recent Results Cancer Res. 2015;204:207-25. doi: 10.1007/978-3-319-22542-5_10. Recent Results Cancer Res. 2015. PMID: 26494391 Review.
-
Long-Term Follow-Up in Medullary Thyroid Carcinoma Patients.Recent Results Cancer Res. 2025;223:267-291. doi: 10.1007/978-3-031-80396-3_11. Recent Results Cancer Res. 2025. PMID: 40102262 Review.
References
-
- Tofail T, Fariduddin M, Haq T, Selim S, Jahan S, Khan MA, Mustari M, Banu H, Alam R, Joarder A. Metastatic medullary thyroid carcinoma with normal serum calcitonin levels. AACE Clin Case Rep. 2018;4(6):e439–e442. doi: 10.4158/ACCR-2017-0260. - DOI
-
- Costante G, Meringolo D, Durante C, Bianchi D, Nocera M, Tumino S, Crocetti U, Attard M, Maranghi M, Torlontano M. Predictive value of serum calcitonin levels for preoperative diagnosis of medullary thyroid carcinoma in a cohort of 5817 consecutive patients with thyroid nodules. J Clin Endocrinol Metab. 2007;92(2):450–455. doi: 10.1210/jc.2006-1590. - DOI - PubMed
-
- Al-Salameh A, Baudry C, Gautier JF, Toubert M-E, Bihan H, Cohen R. Late liver metastasis of medullary thyroid cancer with low calcitonin levels—successfully cured by radiofrequency. Endokrynol Pol. 2016;67(3):326–329. - PubMed
-
- Wells SA, Jr, Asa SL, Dralle H, Elisei R, Evans DB, Gagel RF, Lee N, Machens A, Moley JF, Pacini F. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma: the American Thyroid Association Guidelines Task Force on medullary thyroid carcinoma. Thyroid. 2015;25(6):567–610. doi: 10.1089/thy.2014.0335. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
