

Evaluation of randomized controlled trials: a primer and tutorial for mental health researchers
- PMID: 37649083
- PMCID: PMC10469910
- DOI: 10.1186/s13063-023-07596-3
Evaluation of randomized controlled trials: a primer and tutorial for mental health researchers
Abstract
Background: Considered one of the highest levels of evidence, results of randomized controlled trials (RCTs) remain an essential building block in mental health research. They are frequently used to confirm that an intervention "works" and to guide treatment decisions. Given their importance in the field, it is concerning that the quality of many RCT evaluations in mental health research remains poor. Common errors range from inadequate missing data handling and inappropriate analyses (e.g., baseline randomization tests or analyses of within-group changes) to unduly interpretations of trial results and insufficient reporting. These deficiencies pose a threat to the robustness of mental health research and its impact on patient care. Many of these issues may be avoided in the future if mental health researchers are provided with a better understanding of what constitutes a high-quality RCT evaluation.
Methods: In this primer article, we give an introduction to core concepts and caveats of clinical trial evaluations in mental health research. We also show how to implement current best practices using open-source statistical software.
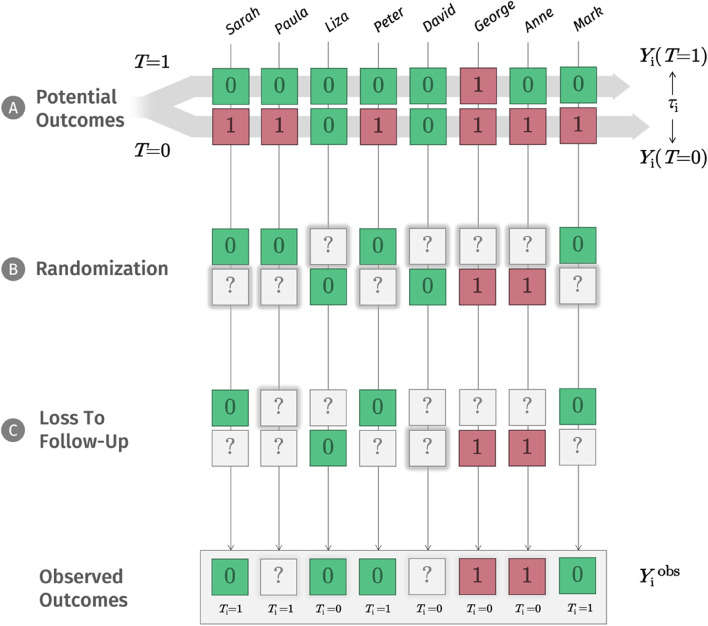
Results: Drawing on Rubin's potential outcome framework, we describe that RCTs put us in a privileged position to study causality by ensuring that the potential outcomes of the randomized groups become exchangeable. We discuss how missing data can threaten the validity of our results if dropouts systematically differ from non-dropouts, introduce trial estimands as a way to co-align analyses with the goals of the evaluation, and explain how to set up an appropriate analysis model to test the treatment effect at one or several assessment points. A novice-friendly tutorial is provided alongside this primer. It lays out concepts in greater detail and showcases how to implement techniques using the statistical software R, based on a real-world RCT dataset.
Discussion: Many problems of RCTs already arise at the design stage, and we examine some avoidable and unavoidable "weak spots" of this design in mental health research. For instance, we discuss how lack of prospective registration can give way to issues like outcome switching and selective reporting, how allegiance biases can inflate effect estimates, review recommendations and challenges in blinding patients in mental health RCTs, and describe problems arising from underpowered trials. Lastly, we discuss why not all randomized trials necessarily have a limited external validity and examine how RCTs relate to ongoing efforts to personalize mental health care.
Keywords: Data analysis; Mental health; Randomized controlled trial; Tutorial.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
DDE is a stakeholder of the Institute for Health Trainings Online (GET.ON), which aims to implement scientific findings related to digital health interventions into routine care.
Figures
Similar articles
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
The Effectiveness of Integrated Care Pathways for Adults and Children in Health Care Settings: A Systematic Review.JBI Libr Syst Rev. 2009;7(3):80-129. doi: 10.11124/01938924-200907030-00001. JBI Libr Syst Rev. 2009. PMID: 27820426
-
Reporting Quality of Randomized Controlled Trials of Periodontal Diseases in Journal Abstracts-A Cross-sectional Survey and Bibliometric Analysis.J Evid Based Dent Pract. 2018 Jun;18(2):130-141.e22. doi: 10.1016/j.jebdp.2017.08.005. Epub 2017 Sep 21. J Evid Based Dent Pract. 2018. PMID: 29747793
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
-
Community first responders for out-of-hospital cardiac arrest in adults and children.Cochrane Database Syst Rev. 2019 Jul 19;7(7):CD012764. doi: 10.1002/14651858.CD012764.pub2. Cochrane Database Syst Rev. 2019. PMID: 31323120 Free PMC article.
Cited by
-
Effectiveness of digital interventions for eight mental disorders: A meta-analytic synthesis.Internet Interv. 2025 Jul 11;41:100860. doi: 10.1016/j.invent.2025.100860. eCollection 2025 Sep. Internet Interv. 2025. PMID: 40703853 Free PMC article. Review.
-
The Communities Organizing for Power Through Empathy (COPE) Community-Based Intervention to Improve Adult Mental Health During Disasters and Crises: Protocol for a Stepped-Wedge Cluster Randomized Trial.JMIR Res Protoc. 2025 May 20;14:e63723. doi: 10.2196/63723. JMIR Res Protoc. 2025. PMID: 40392582 Free PMC article.
-
Additive effects of adjunctive app-based interventions for mental disorders - A systematic review and meta-analysis of randomised controlled trials.Internet Interv. 2023 Dec 18;35:100703. doi: 10.1016/j.invent.2023.100703. eCollection 2024 Mar. Internet Interv. 2023. PMID: 38225971 Free PMC article. Review.
-
The overestimation of the effect sizes of psychotherapies for depression in waitlist controlled trials: a meta-analytic comparison with usual care controlled trials.Epidemiol Psychiatr Sci. 2024 Nov 6;33:e56. doi: 10.1017/S2045796024000611. Epidemiol Psychiatr Sci. 2024. PMID: 39501660 Free PMC article.
-
Evaluating the Practicality of Causal Inference From Non-randomized Observational Data in Small-Scale Clinical Settings: A Study on the Effects of Ninjin'yoeito.Cureus. 2024 Mar 8;16(3):e55825. doi: 10.7759/cureus.55825. eCollection 2024 Mar. Cureus. 2024. PMID: 38463406 Free PMC article.
References
-
- Howick J, Chalmers I, Glasziou P, Greenhalgh T, Heneghan C, Liberati A, Moschetti I, Phillips B, Thornton H. The 2011 Oxford CEBM evidence levels of evidence (introductory document). Oxf Cent Evid Based Med. 2011. http://www.cebm.net/index.aspx?o=5653.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
