

The screening, identification, design and clinical application of tumor-specific neoantigens for TCR-T cells
- PMID: 37649123
- PMCID: PMC10466891
- DOI: 10.1186/s12943-023-01844-5
The screening, identification, design and clinical application of tumor-specific neoantigens for TCR-T cells
Abstract
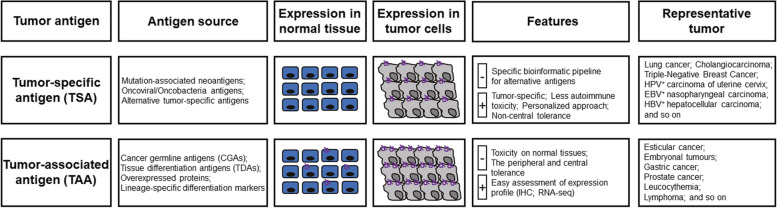
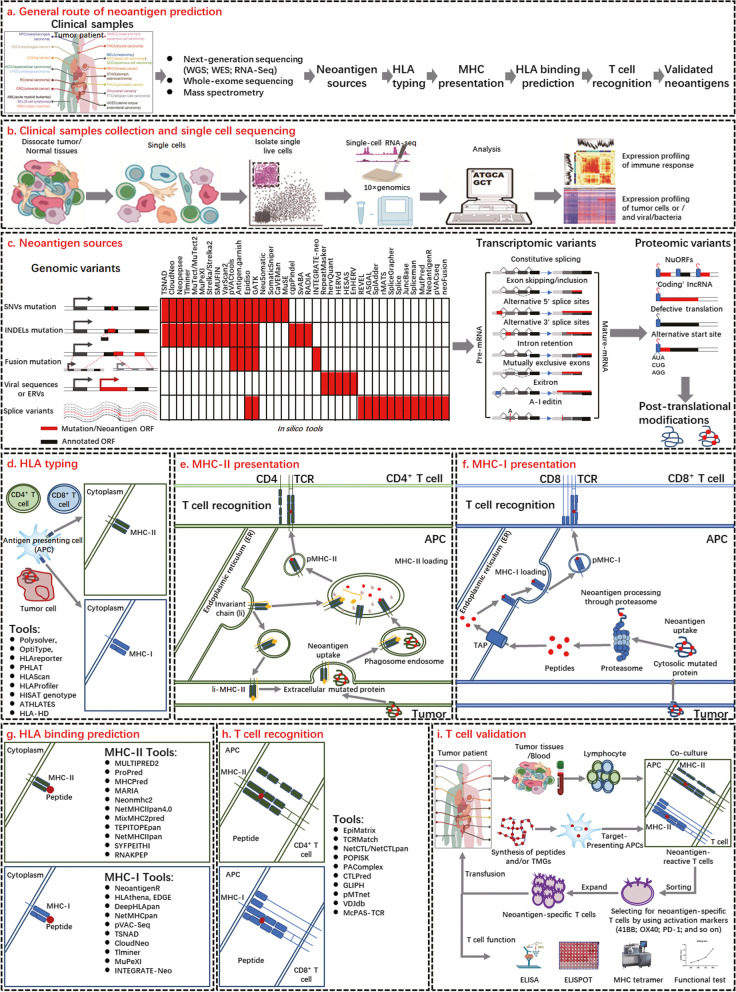
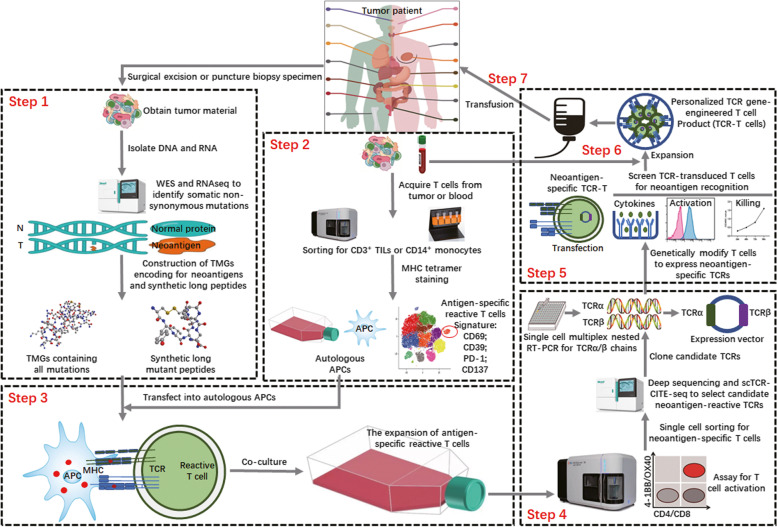
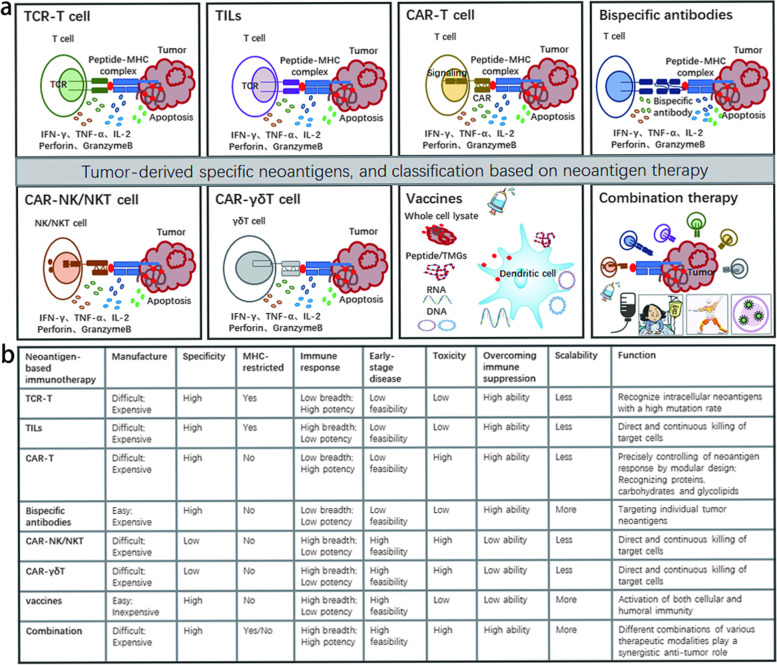
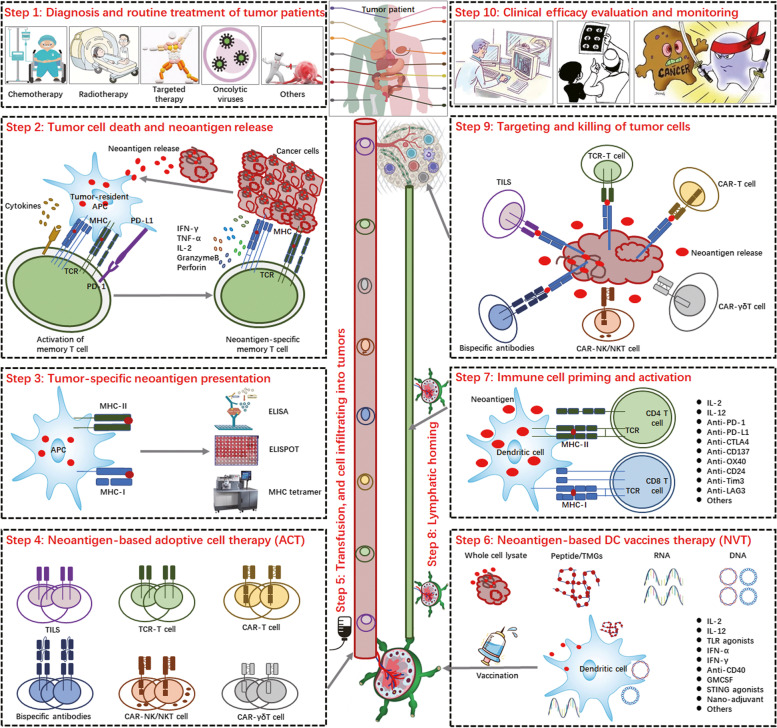
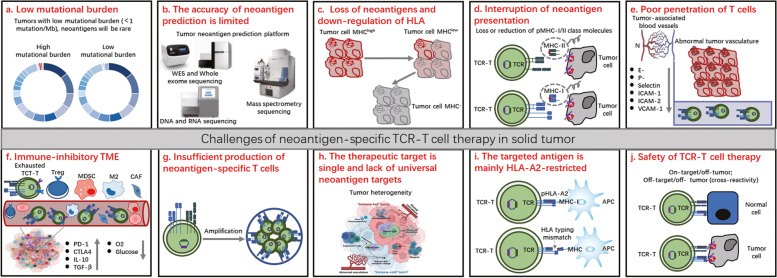
Recent advances in neoantigen research have accelerated the development of tumor immunotherapies, including adoptive cell therapies (ACTs), cancer vaccines and antibody-based therapies, particularly for solid tumors. With the development of next-generation sequencing and bioinformatics technology, the rapid identification and prediction of tumor-specific antigens (TSAs) has become possible. Compared with tumor-associated antigens (TAAs), highly immunogenic TSAs provide new targets for personalized tumor immunotherapy and can be used as prospective indicators for predicting tumor patient survival, prognosis, and immune checkpoint blockade response. Here, the identification and characterization of neoantigens and the clinical application of neoantigen-based TCR-T immunotherapy strategies are summarized, and the current status, inherent challenges, and clinical translational potential of these strategies are discussed.
Keywords: ACT; Immunotherapy; Neoantigen; TCR-T; TSA.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Neoantigens: promising targets for cancer therapy.Signal Transduct Target Ther. 2023 Jan 6;8(1):9. doi: 10.1038/s41392-022-01270-x. Signal Transduct Target Ther. 2023. PMID: 36604431 Free PMC article. Review.
-
Advances in identification and selection of personalized neoantigen/T-cell pairs for autologous adoptive T cell therapies.Oncoimmunology. 2021 Jan 7;10(1):1869389. doi: 10.1080/2162402X.2020.1869389. Oncoimmunology. 2021. PMID: 33520408 Free PMC article. Review.
-
Virus-like particle-mediated delivery of structure-selected neoantigens demonstrates immunogenicity and antitumoral activity in mice.J Transl Med. 2024 Jan 3;22(1):14. doi: 10.1186/s12967-023-04843-8. J Transl Med. 2024. PMID: 38172991 Free PMC article.
-
The role of neoantigens in tumor immunotherapy.Biomed Pharmacother. 2022 Jul;151:113118. doi: 10.1016/j.biopha.2022.113118. Epub 2022 May 24. Biomed Pharmacother. 2022. PMID: 35623169 Review.
-
Neoantigen identification strategies enable personalized immunotherapy in refractory solid tumors.J Clin Invest. 2019 Mar 5;129(5):2056-2070. doi: 10.1172/JCI99538. Print 2019 May 1. J Clin Invest. 2019. PMID: 30835255 Free PMC article.
Cited by
-
The development and application of chimeric antigen receptor natural killer (CAR-NK) cells for cancer therapy: current state, challenges and emerging therapeutic advances.Exp Hematol Oncol. 2024 Dec 4;13(1):118. doi: 10.1186/s40164-024-00583-7. Exp Hematol Oncol. 2024. PMID: 39633491 Free PMC article. Review.
-
A case of response to combination treatment with TSA-DC-CTL immunotherapy and osimertinib in EGFR mutated advanced lung adenocarcinoma.Mol Cancer. 2024 Aug 9;23(1):163. doi: 10.1186/s12943-024-02070-3. Mol Cancer. 2024. PMID: 39123231 Free PMC article.
-
Immunotherapy for glioblastoma: current state, challenges, and future perspectives.Cell Mol Immunol. 2024 Dec;21(12):1354-1375. doi: 10.1038/s41423-024-01226-x. Epub 2024 Oct 15. Cell Mol Immunol. 2024. PMID: 39406966 Free PMC article. Review.
-
Navigating the Immune Maze: Pioneering Strategies for Unshackling Cancer Immunotherapy Resistance.Cancers (Basel). 2023 Dec 15;15(24):5857. doi: 10.3390/cancers15245857. Cancers (Basel). 2023. PMID: 38136402 Free PMC article. Review.
-
Harnessing innate immunity against glioblastoma microenvironment.Front Immunol. 2025 Jul 25;16:1648601. doi: 10.3389/fimmu.2025.1648601. eCollection 2025. Front Immunol. 2025. PMID: 40787444 Free PMC article. Review.
References
-
- Disis M, Guthrie KA, Liu Y, Coveler AL, Higgins DM, Childs JS, Dang Y, Salazar LG. Safety and outcomes of a plasmid DNA vaccine encoding the ERBB2 intracellular domain in patients with advanced-stage ERBB2-positive breast cancer: a phase 1 nonrandomized clinical trial. JAMA Oncol. 2023;9:71–78. - PMC - PubMed
-
- Gao T, Cen Q, Lei H. A review on development of MUC1-based cancer vaccine. Biomed Pharmacother. 2020;132:110888. - PubMed
-
- Ellingsen EB, Aamdal E, Guren T, Lilleby W, Brunsvig PF, Mangsbo SM, Aamdal S, Hovig E, Mensali N, Gaudernack G, Inderberg EM. Durable and dynamic hTERT immune responses following vaccination with the long-peptide cancer vaccine UV1: long-term follow-up of three phase I clinical trials. J Immunother Cancer. 2022;10(5):e004345. - PMC - PubMed
-
- Hegde PS, Chen DS. Top 10 challenges in cancer immunotherapy. Immunity. 2020;52:17–35. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
