

Unveiling a Shared Precursor Condition for Acne Keloidalis Nuchae and Primary Cicatricial Alopecias
- PMID: 37649568
- PMCID: PMC10464825
- DOI: 10.2147/CCID.S422310
Unveiling a Shared Precursor Condition for Acne Keloidalis Nuchae and Primary Cicatricial Alopecias
Abstract
Purpose: Small observational studies suggest subclinical disease occurrence in the normal-appearing scalp zones of several primary cicatricial alopecias. To aid patient management, we began routinely evaluating the entire scalp of patients with acne keloidalis nuchae (AKN), including trichoscopy-guided biopsies.
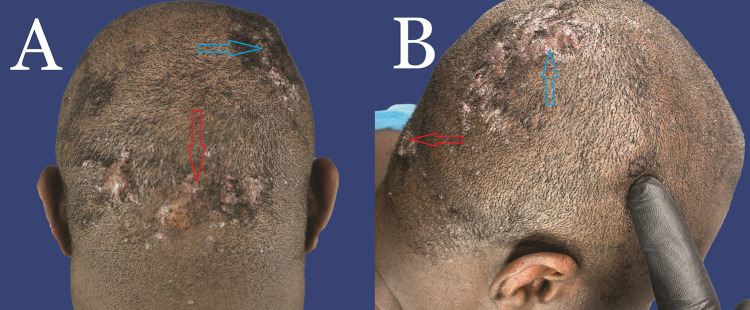
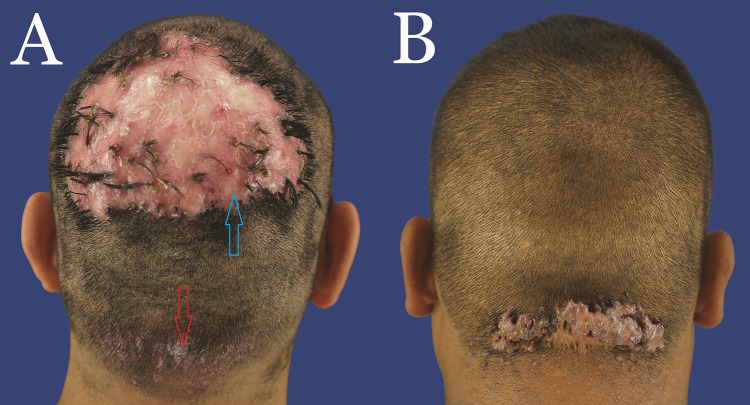
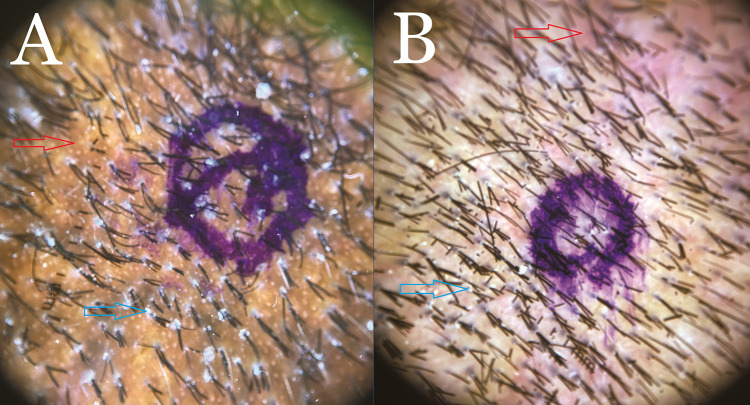
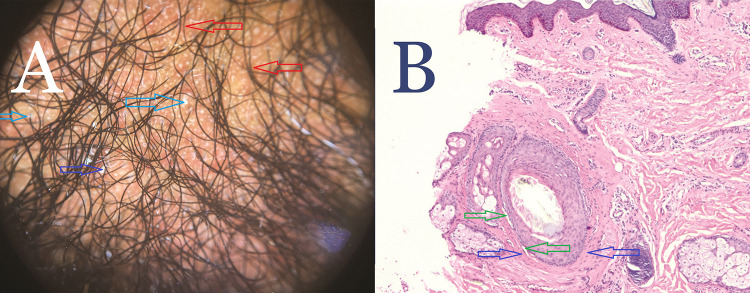
Patients and methods: This retrospective study evaluated 41 patients sequentially presenting with AKN at a single clinic between June and December 2022. Primary lesions and normal-appearing scalp in the superior parietal scalp at least 5 cm away from AKN-affected zones were clinically evaluated, and areas showing perifollicular erythema or scales/casts on trichoscopy were biopsied and histologically analyzed.
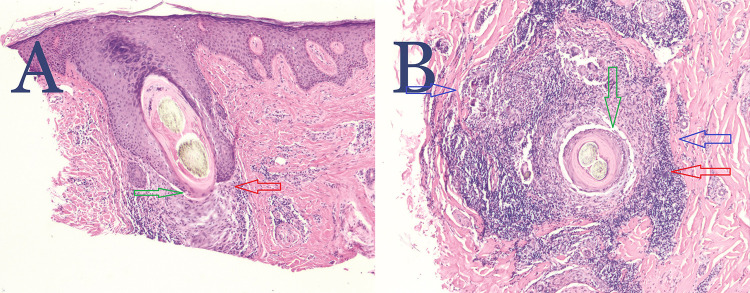
Results: Forty-one men with AKN, including 20 men of African descent, 17 Hispanic, and 4 European-descended Whites, were evaluated. All patients, including 22% with associated folliculitis decalvans, showed scalp-wide trichoscopy signs of perifollicular erythema or scaling in normal-appearing scalp areas. All patients showed histologic evidence of perifollicular infundibulo-isthmic lymphocytoplasmic infiltrates and fibrosis (PIILIF), with 96% showing Vellus or miniaturized hair absence. PIILIF was often clinically mistaken for seborrheic dermatitis (44-51%). All White patients had mild papular acne keloidalis nuchae lesions mistaken for seborrheic dermatitis.
Conclusion: PIILIF may be a precursor to a wide spectrum of primary cicatricial alopecias, including AKN and folliculitis decalvans. This finding carries implications for the early diagnosis and management of AKN and other primary cicatricial alopecias.
Keywords: central centrifugal cicatricial alopecia; folliculitis decalvans; frontal fibrosing alopecia; lichen planopilaris; scarring alopecia; subclinical.
Plain language summary
Acne keloidalis nuchae (AKN) is a type of hair loss and scalp condition marked by scarring and inflammation. This condition falls under a group of chronic hair and scalp issues known as primary cicatricial alopecia (PCA). Current treatments for AKN and similar PCAs often do not work well, and the condition tends to return. We have found a hidden scalp condition that could be causing AKN and other PCAs. It’s a subtle disease that affects the entire scalp, even though it might not show noticeable symptoms. We have observed this condition in all 41 AKN patients in our study, and it’s characterized by certain changes in the hair and scalp’s structure and immune system response. Other studies have linked this condition to various other PCAs. We believe this hidden condition could be causing AKN and making it come back after treatment. This study suggests that treating AKN might require a broader approach beyond just treating the visible symptoms. Since this hidden condition exists in other PCAs, it might be a common cause.
© 2023 Umar et al.
Conflict of interest statement
Sanusi Umar owned shares and issued patents and patent applications in FineTouch Laboratories Inc. and Dr. U Devices Inc. at the time of this work. The other authors declare that they have no conflicts of interest in this work.
Figures

Similar articles
-
Naked Hair Shafts as a Marker of Cicatricial Alopecia.Am J Dermatopathol. 2018 Jul;40(7):498-501. doi: 10.1097/DAD.0000000000001075. Am J Dermatopathol. 2018. PMID: 29293128
-
[Translated article] Acne Keloidalis Nuchae: A Therapeutic Challenge for Dermatologists.Actas Dermosifiliogr. 2025 Apr;116(4):T394-T402. doi: 10.1016/j.ad.2025.02.015. Epub 2025 Feb 11. Actas Dermosifiliogr. 2025. PMID: 39947588 Review. English, Spanish.
-
Hair and Nail Conditions: Alopecia Evaluation.FP Essent. 2022 Jun;517:11-16. FP Essent. 2022. PMID: 35679467
-
Primary scarring alopecias.Curr Probl Dermatol. 2015;47:76-86. doi: 10.1159/000369407. Epub 2015 Feb 20. Curr Probl Dermatol. 2015. PMID: 26370646 Review.
-
Scarring Alopecia.Dermatol Clin. 2023 Jul;41(3):519-537. doi: 10.1016/j.det.2023.02.007. Epub 2023 Apr 14. Dermatol Clin. 2023. PMID: 37236719 Review.
Cited by
-
Refractory Folliculitis Decalvans Treatment Success with a Novel Surgical Excision Approach Using Guarded High-Tension Sutures.Clin Cosmet Investig Dermatol. 2023 Sep 1;16:2381-2390. doi: 10.2147/CCID.S422077. eCollection 2023. Clin Cosmet Investig Dermatol. 2023. PMID: 37675182 Free PMC article.
References
-
- Dinehart SM, Tanner L, Mallory SB, Herzberg AJ. Acne keloidalis in women. Cutis. 1989;44(3):250–252. - PubMed
