

Evaluation of FAPI PET imaging in gastric cancer: a systematic review and meta-analysis
- PMID: 37649615
- PMCID: PMC10465231
- DOI: 10.7150/thno.88335
Evaluation of FAPI PET imaging in gastric cancer: a systematic review and meta-analysis
Abstract
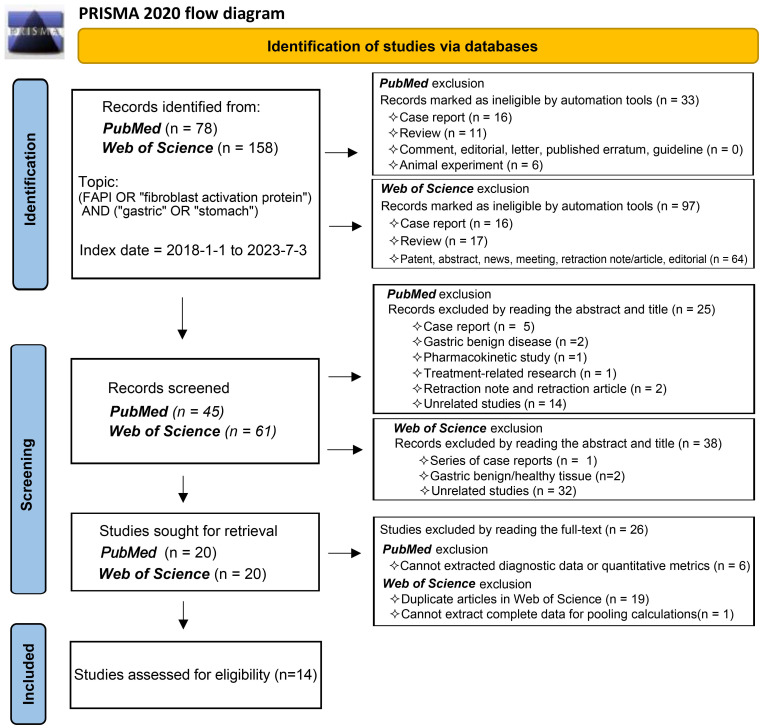
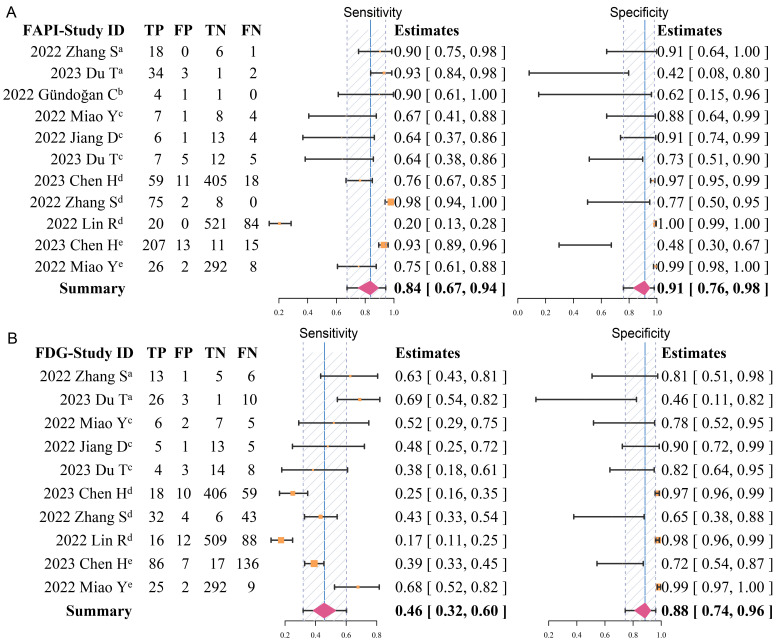
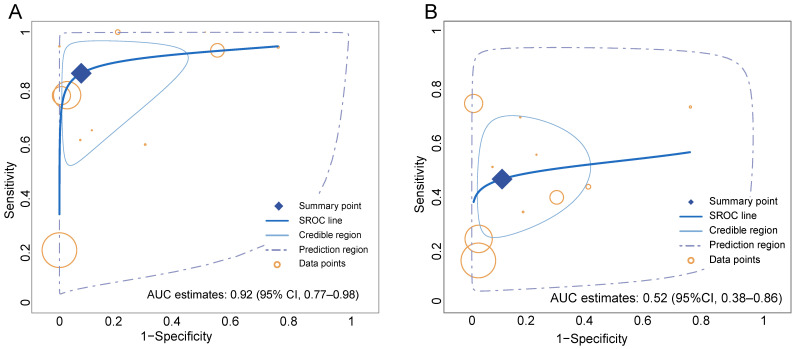
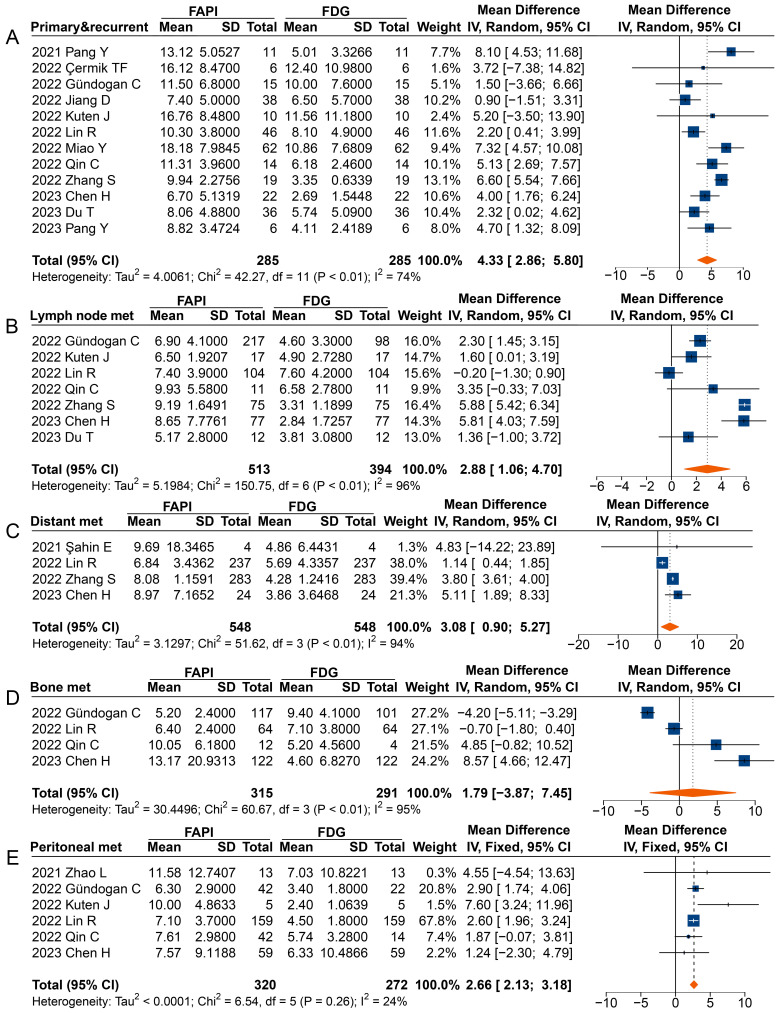
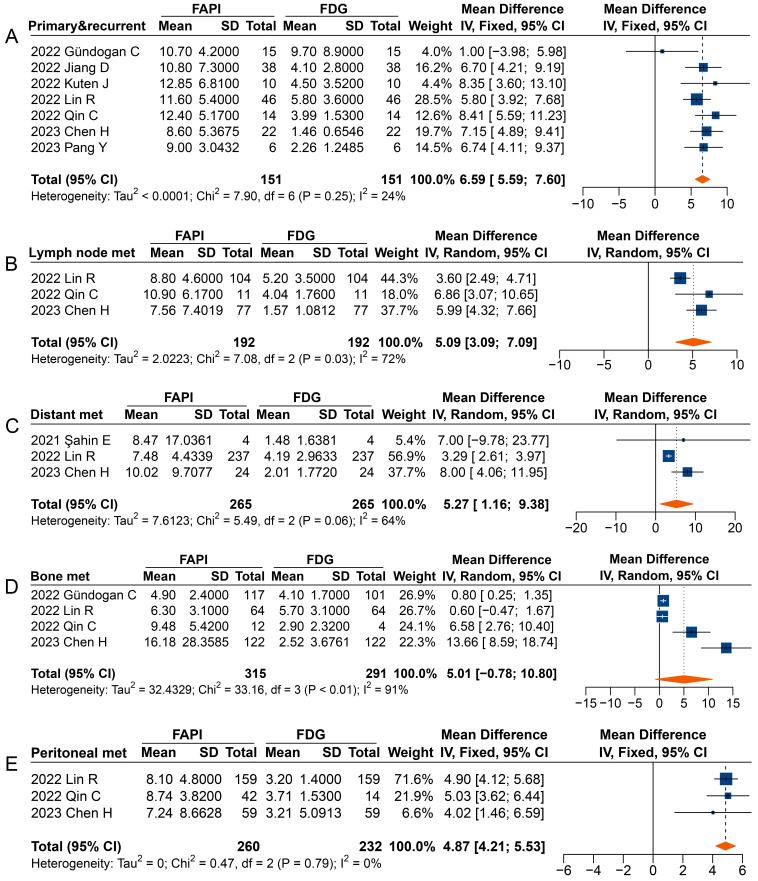
Purpose: Recent studies suggest that 68Ga-FAPI PET/CT demonstrated superiority over 18F-FDG PET/CT in the evaluation of various cancer types, especially in gastric cancer (GC). By comprehensively reviewing and analysing the differences between 68Ga-FAPI and 18F-FDG in GC, some evidence is provided to foster the broader clinical application of FAPI PET imaging. Methods: In this review, studies published up to July 3, 2023, that employed radionuclide labelled FAPI as a diagnostic radiotracer for PET in GC were analysed. These studies were sourced from both the PubMed and Web of Science databases. Our statistical analysis involved a bivariate meta-analysis of the diagnostic data and a meta-analysis of the quantitative metrics. These were performed using R language. Results: The meta-analysis included 14 studies, with 527 patients, of which 358 were diagnosed with GC. Overall, 68Ga-FAPI showed higher pooled sensitivity (0.84 [95% CI 0.67-0.94] vs. 0.46 [95% CI 0.32-0.60]), specificity (0.91 [95% CI 0.76-0.98] vs. 0.88 [95% CI 0.74-0.96]) and area under the curve (AUC) (0.92 [95% CI 0.77-0.98] vs. 0.52 [95% CI 0.38-0.86]) than 18F-FDG. The evidence showed superior pooled sensitivities of 68Ga-FAPI PET over 18F-FDG for primary tumours, local recurrence, lymph node metastases, distant metastases, and peritoneal metastases. Furthermore, 68Ga-FAPI PET provided higher maximum standardized uptake value (SUVmax) and tumour-to-background ratios (TBR). For bone metastases, while 68Ga-FAPI PET demonstrated slightly lower patient-based pooled sensitivity (0.93 vs. 1.00), it significantly outperformed 18F-FDG in the lesion-based analysis (0.95 vs. 0.65). However, SUVmax (mean difference [MD] 1.79 [95% CI -3.87-7.45]) and TBR (MD 5.01 [95% CI -0.78-10.80]) of bone metastases showed no significant difference between 68Ga-FAPI PET/CT and 18F-FDG PET/CT. Conclusion: Compared with 18F-FDG, 68Ga-FAPI PET imaging showed improved diagnostic accuracy in the evaluation of GC. It can be effectively applied to the early diagnosis, initial staging, and detection of recurrence/metastases of GC. 68Ga-FAPI may have the potential of replacing 18F-FDG in GC in future applications.
Keywords: 18F-FDG; 68Ga-FAPI; PET/CT; fibroblast activation protein; gastric cancer.
© The author(s).
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures
Similar articles
-
Usefulness of [68Ga]FAPI-04 and [18F]FDG PET/CT for the detection of primary tumour and metastatic lesions in gastrointestinal carcinoma: a comparative study.Eur Radiol. 2023 Apr;33(4):2779-2791. doi: 10.1007/s00330-022-09251-y. Epub 2022 Nov 17. Eur Radiol. 2023. PMID: 36394603
-
Superiority of [68Ga]Ga-FAPI-04/[18F]FAPI-42 PET/CT to [18F]FDG PET/CT in delineating the primary tumor and peritoneal metastasis in initial gastric cancer.Eur Radiol. 2022 Sep;32(9):6281-6290. doi: 10.1007/s00330-022-08743-1. Epub 2022 Apr 5. Eur Radiol. 2022. Retraction in: Eur Radiol. 2023 Jun;33(6):4511. doi: 10.1007/s00330-022-09386-y. PMID: 35380229 Retracted.
-
Comparison of [68Ga]Ga-FAPI and [18F]FDG uptake in patients with gastric signet-ring-cell carcinoma: a multicenter retrospective study.Eur Radiol. 2023 Feb;33(2):1329-1341. doi: 10.1007/s00330-022-09084-9. Epub 2022 Aug 17. Eur Radiol. 2023. PMID: 35976396
-
Head to head comparison of 68Ga-FAPI PET/CT with 18F-FDG PET/CT in primary and metastatic lesions of gastric tumor: A systematic review and meta-analysis.Hell J Nucl Med. 2024 Jan-Apr;27(1):35-45. doi: 10.1967/s002449912703. Epub 2024 Apr 18. Hell J Nucl Med. 2024. PMID: 38629816
-
Comparison of 18F-fluorodeoxyglucose PET and 68Ga-fibroblast Activation Protein Inhibitor PET in Head and Neck Cancers: A Systematic Review and Meta-analysis.Acad Radiol. 2025 Aug;32(8):4818-4828. doi: 10.1016/j.acra.2025.02.038. Epub 2025 Mar 10. Acad Radiol. 2025. PMID: 40068998
Cited by
-
Comparison of Al[18F]-NOTA-FAPI-04 PET/CT and [18F]-FDG PET/CT in a patient with lung cancer and pulmonary tuberculosis: a case report and literature review.Front Oncol. 2025 Feb 3;15:1470132. doi: 10.3389/fonc.2025.1470132. eCollection 2025. Front Oncol. 2025. PMID: 39963103 Free PMC article.
-
Evaluating the diagnostic performance of [18F]ALF-NOTA-FAPI-04 PET/CT in gastric cancer: a comparative study with [18F]FDG PET/CT.Eur Radiol. 2025 Jun;35(6):3314-3323. doi: 10.1007/s00330-024-11219-z. Epub 2024 Nov 28. Eur Radiol. 2025. PMID: 39604653 Free PMC article.
-
Rapid and specific immunoPET imaging of Nectin-4 in gastric cancer and non-small cell lung cancer using [64Cu]Cu-NOTA-EV-F(ab')2.Eur J Nucl Med Mol Imaging. 2025 Jun 21:10.1007/s00259-025-07402-z. doi: 10.1007/s00259-025-07402-z. Online ahead of print. Eur J Nucl Med Mol Imaging. 2025. PMID: 40542857
-
Strategies for specific multimodal imaging of cancer-associated fibroblasts and applications in theranostics of cancer.Mater Today Bio. 2024 Dec 24;30:101420. doi: 10.1016/j.mtbio.2024.101420. eCollection 2025 Feb. Mater Today Bio. 2024. PMID: 39839493 Free PMC article. Review.
-
Non-invasive liquid biopsy based on transcriptomic profiling for early diagnosis of occult peritoneal metastases in locally advanced gastric cancer.NPJ Precis Oncol. 2025 Apr 15;9(1):109. doi: 10.1038/s41698-025-00875-z. NPJ Precis Oncol. 2025. PMID: 40234664 Free PMC article.
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A. et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71:209–49. - PubMed
-
- Ajani JA, D'Amico TA, Bentrem DJ, Chao J, Cooke D, Corvera C. et al. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022;20:167–92. - PubMed
-
- Lauren P. The Two Histological Main Types of Gastric Carcinoma: Diffuse and So-Called Intestinal-Type Carcinoma. An Attempt at a Histo-Clinical Classification. Acta Pathol Microbiol Scand. 1965;64:31–49. - PubMed
-
- Chen YC, Fang WL, Wang RF, Liu CA, Yang MH, Lo SS. et al. Clinicopathological Variation of Lauren Classification in Gastric Cancer. Pathol Oncol Res. 2016;22:197–202. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
