Effect of rScO2-Guided Blood Pressure Management on Postoperative Complications in Elderly Patients After Major Noncardiac Surgery: Protocol for a Randomized Controlled Trial
- PMID: 37649853
- PMCID: PMC10464896
- DOI: 10.2147/IJGM.S426245
Effect of rScO2-Guided Blood Pressure Management on Postoperative Complications in Elderly Patients After Major Noncardiac Surgery: Protocol for a Randomized Controlled Trial
Abstract
Background: Postoperative complications are common after major surgical procedures, leading to increased morbidity and mortality. Regional cerebral oxygen saturation (rScO2) reflects cerebral and global perfusion, and thus it can be used to guide hemodynamic management. We aim to explore the effect of rScO2-guided blood pressure management strategy on postoperative major complications in older adults who undergo major noncardiac surgery.
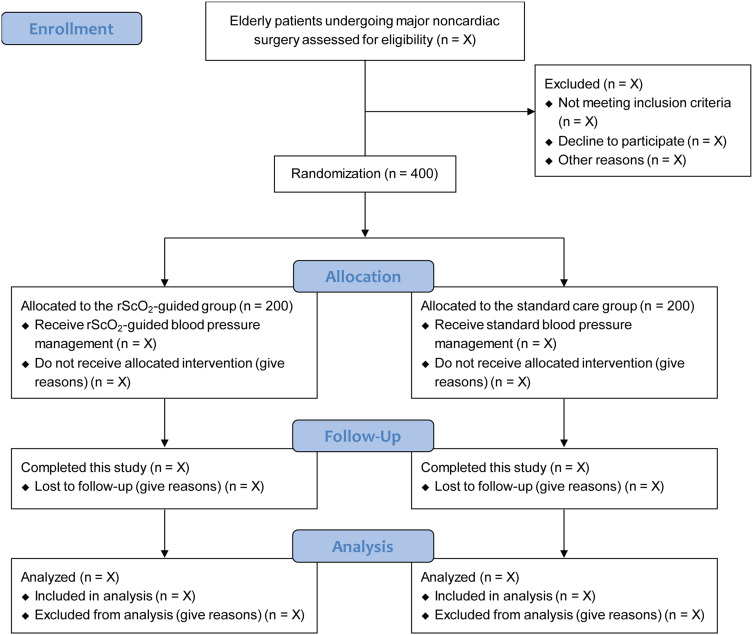
Methods: This randomized controlled clinical trial includes a total of 400 elderly patients receiving major noncardiac surgery and general anesthesia. Patients will be randomized (1:1) to one of two blood pressure management groups: a standard care group (targeting mean arterial pressure >65 mmHg or within 20% of baseline value), and a rScO2-guided group (absolute value of rScO2 >60% or decrease in rScO2 <10% of baseline). The primary outcome is the composite outcome of major complications (including infectious, respiratory, neurologic, cardiovascular, renal, thromboembolic gastrointestinal, and surgical complications) and deaths within the first 7 days after surgery. Secondary outcomes include the individual components of the primary outcome by day 7 after surgery and 30-day mortality. Data will be analyzed in the modified intention-to-treat population.
Discussion: This study will provide evidence for improving postoperative outcomes using the rScO2-guided blood pressure management among older adults who undergo major noncardiac surgery.
Trial registration: Chinese Clinical Trial Registry (Identifier: ChiCTR2200060816).
Keywords: blood pressure management; elderly patients; major noncardiac surgery; postoperative major complications; regional cerebral oxygen saturation.
Plain language summary
This is a protocol for a prospective, randomized, controlled clinical trial to evaluate the use of intraoperative individualized regional cerebral oxygen saturation (rScO2) optimization for blood pressure management in older adults undergoing major noncardiac surgery. The primary focus of this trial is the composite outcome of major complications (including infectious, respiratory, neurologic, cardiovascular, renal, thromboembolic gastrointestinal, and surgical complications) and deaths within the first 7 days after surgery. The secondary outcomes are the individual components of the primary outcome by day 7 after surgery and 30-day mortality. The findings of this trial will provide clinical evidence for the rScO2-guided blood pressure management to improve postoperative outcomes in older patients who are scheduled for major noncardiac surgery.
© 2023 Yang et al.
Conflict of interest statement
The authors have no conflicts of interest to declare.