

A Health State Utility Study to Elicit Societal Values Associated with Pulmonary Hypertension
- PMID: 37650045
- PMCID: PMC10464901
- DOI: 10.2147/PPA.S400061
A Health State Utility Study to Elicit Societal Values Associated with Pulmonary Hypertension
Abstract
Aim: Pulmonary hypertension (PH) is a rare, severe, and progressive pulmonary vascular disease, which includes five subgroups with similar presentation. Symptoms include dyspnea, and fatigue, and can significantly impact one's health-related quality of life (HRQL). Although treatments are mainly medical, PH group 4, chronic thromboembolic pulmonary hypertension (CTEPH), can be managed with procedures, ie pulmonary endarterectomy (PEA) and balloon pulmonary angioplasty (BPA). Currently, drugs in Europe are only approved for pulmonary arterial hypertension (PAH), and CTEPH therefore the aim of this study was to elicit novel societal health state utilities in the UK for PAH and CTEPH based on disease severity, functional class (FC), clinical events, and treatment procedures specifically for CTEPH.
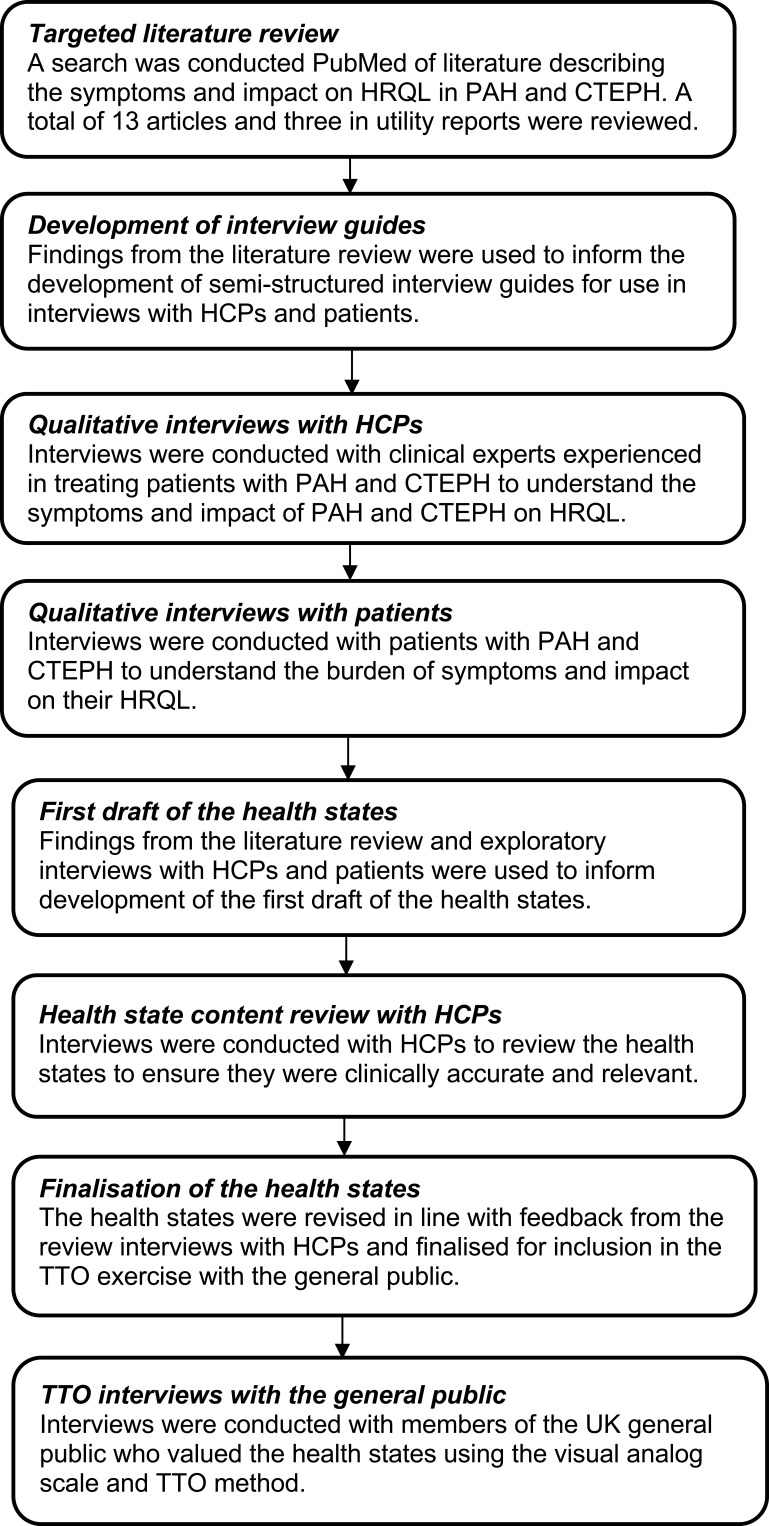
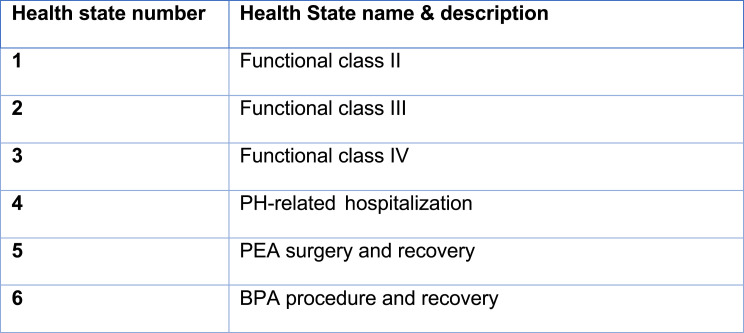
Material and methods: Six health states were defined: World Health Organization (WHO)-FC II, WHO-FC III, and WHO-FC IV [defined by the New York Heart Association (NYHA)]; PH-related hospitalization; and "BPA procedure and recovery" and "PEA surgery and recovery". Health states were based on a targeted literature review and two rounds of interviews with clinical experts (N = 4) and patients (N = 6). Draft health states were validated in cognitive debriefing interviews with clinical experts (N = 3). Health states were valued by the UK general public (n = 200), using a visual analogue scale (VAS) and time trade-off (TTO) assessment with the lead time method.
Results: The mean TTO values/utilities were 0.81 (FC II), 0.80 (BPA), 0.78 (PEA), 0.59 (FC III), 0.28 (FC IV), and 0.25 (PH-related hospitalization). Each progression in FC was associated with worse TTO scores.
Conclusion: This study reports societal utility values for PAH and CTEPH in the UK. It provides first utility estimates for states such as BPA procedure and recovery, PEA surgery and recovery and PH-related hospitalization for this population. The results show important distinctions between FC, treatment procedures, and hospitalization, and the significant burden of disease on HRQL.
Keywords: CTEPH; PAH; health-related quality of life; hospitalization; time trade-off; vignette.
© 2023 Nafees et al.
Conflict of interest statement
BN and HMdF were paid by Actelion Pharmaceuticals Ltd to conduct the research. AB is an employee of Actelion Pharmaceuticals Ltd, a Janssen Pharmaceutical Company of Johnson & Johnson. ET is an employee of Janssen Global Commercial Strategy Organization, High Wycombe, UK. WGS has received honoraria for speaking and consultation from Actelion Pharmaceuticals Ltd, a Janssen Pharmaceutical Company of Johnson and Johnson, Acceleron, Bayer, Gossamer Bio, and MSD. The authors report no other conflicts of interest in this work.
Figures
References
-
- Galie N, Humbert M, Vachiery L, et al; 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. The joint task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Eur Heart J. 2015. doi: 10.1093/eurheartj/ehv317 - DOI
LinkOut - more resources
Full Text Sources
