

Real-World Effectiveness and Safety of a Single-Pill Combination of Olmesartan/Amlodipine/Hydrochlorothiazide in Korean Patients with Hypertension and Cardiovascular Risk Factors
- PMID: 37651078
- PMCID: PMC10567848
- DOI: 10.1007/s12325-023-02632-9
Real-World Effectiveness and Safety of a Single-Pill Combination of Olmesartan/Amlodipine/Hydrochlorothiazide in Korean Patients with Hypertension and Cardiovascular Risk Factors
Abstract
Introduction: Patients with hypertension and additional cardiovascular risk factors pose a challenge by requiring more intensive blood pressure (BP) control. Single-pill combination (SPC) therapy can benefit these patients by improving medication adherence.
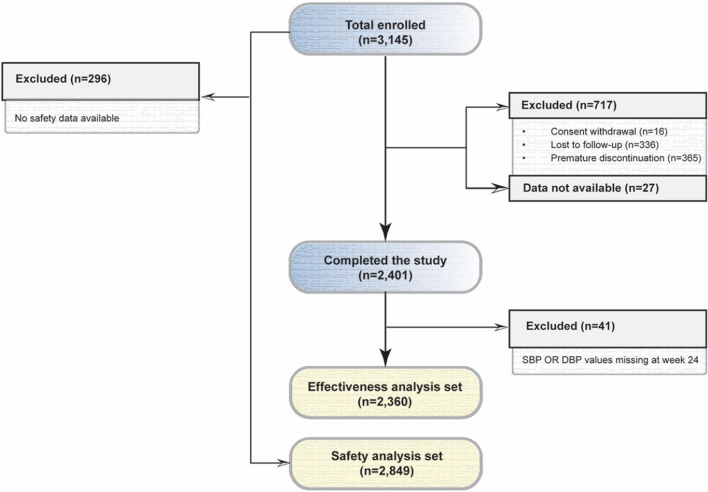
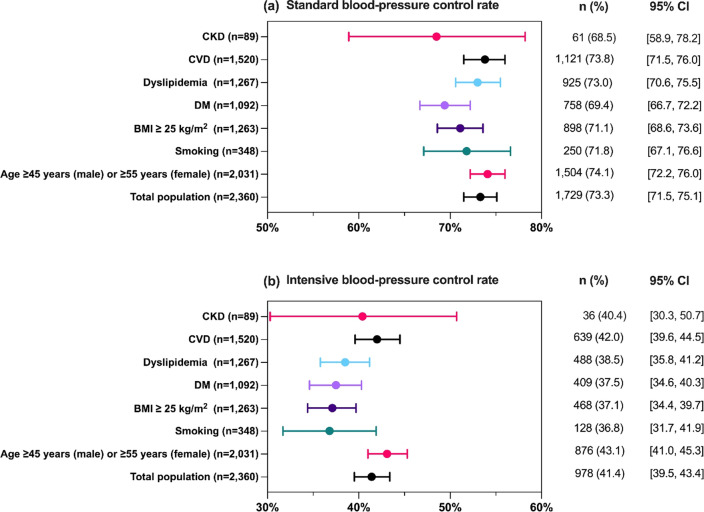
Methods: This prospective, multicenter observational study assessed the real-world safety and effectiveness of an SPC containing olmesartan, amlodipine, and hydrochlorothiazide (O/A/H) in South Korean patients with hypertension and cardiovascular risk factors. BP control rates, defined as the percentage of patients achieving systolic BP (SBP) < 130 mmHg and diastolic BP (DBP) < 80 mmHg for intensive BP control, and < 140 mmHg and < 90 mmHg, respectively, for standard BP control, were investigated across various cardiovascular risk groups, along with changes in SBP and DBP from baseline to week 24.
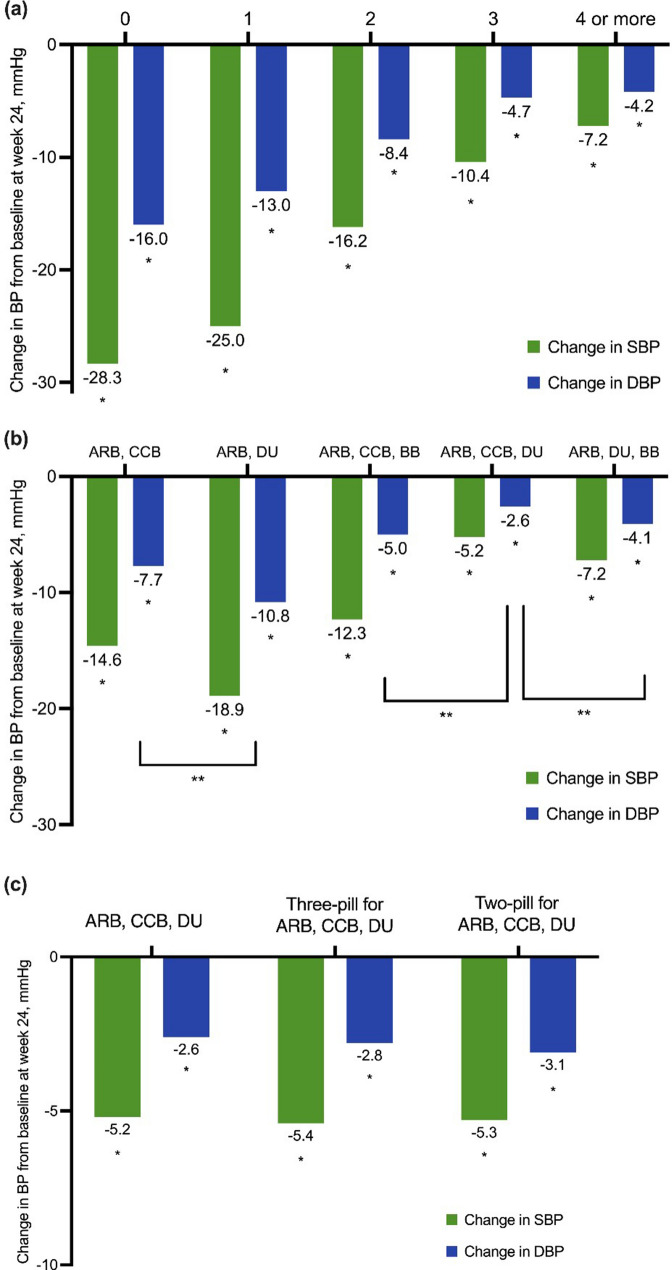
Results: The most prevalent cardiovascular risk factor was age (≥ 45 years in men, ≥ 55 years in women, 86.1%), followed by cardiovascular diseases (64.4%), dyslipidemia (53.7%), body mass index ≥ 25 kg/m2 (53.5%), and diabetes mellitus (DM) (46.3%). Switching to O/A/H showed significant BP reduction, with a mean change of - 17.8 mmHg/- 9.3 mmHg in SBP/DBP within 4 weeks. The intensive BP control rate was 41.4% (95% confidence interval [CI] 39.5, 43.4), and the standard BP control rate was 73.3% (95% CI 71.5, 75.1), with better control rates in the risk age group (43.1% and 74.1%, respectively) and cardiovascular disease group (42.0% and 73.8%, respectively). The DM group had relatively lower control rates (37.5% for intensive control and 69.4% for standard control). Common adverse drug reactions included dizziness (2.91%), hypotension (1.51%), and headaches (0.70%).
Conclusion: The SPC therapy of O/A/H caused a rapid and sustained reduction in SBP/DBP in patients' hypertension and additional cardiovascular risk factors. The therapy was safe and well tolerated.
Study registration number: KCT0003401 ( https://cris.nih.go.kr/cris/search/detailSearch.do/20795 ).
Keywords: Olmesartan-based combination therapy; Patients with hypertension and additional cardiovascular risk factors; Real-world effectiveness of blood pressure control; Single-pill combination.
© 2023. The Author(s).
Conflict of interest statement
Jaewon Oh, Wonho Kim, Gee-Hee Kim, Hack-Lyoung Kim, Sang-Don Park, Kyung Wan Min, Dongkeun Hyun, Jun Hwa Hong, and Soo Lim declare that they have no competing interests. Jinho Shin received honoraria from Daiichi Sankyo, Organon, Bristol Myers Squibb, Menarini, Sanofi, Hanmi, Boryung, Chong Kun Dang, and Daewoong and grants from Sanofi and Hanmi.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
