

Clinical and Immunologic Correlates of Vasodilatory Shock Among Ebola Virus-Infected Nonhuman Primates in a Critical Care Model
- PMID: 37652048
- PMCID: PMC10651209
- DOI: 10.1093/infdis/jiad374
Clinical and Immunologic Correlates of Vasodilatory Shock Among Ebola Virus-Infected Nonhuman Primates in a Critical Care Model
Abstract
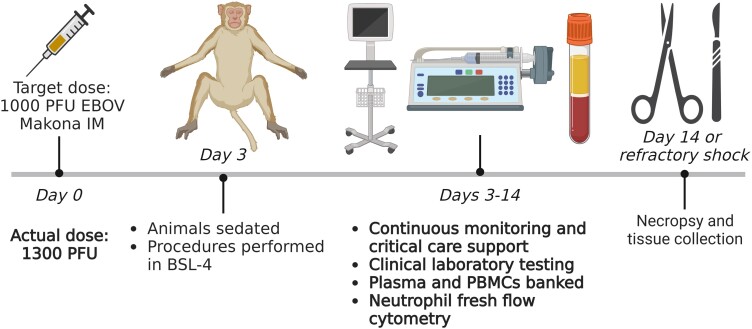
Background: Existing models of Ebola virus infection have not fully characterized the pathophysiology of shock in connection with daily virologic, clinical, and immunologic parameters. We implemented a nonhuman primate critical care model to investigate these associations.
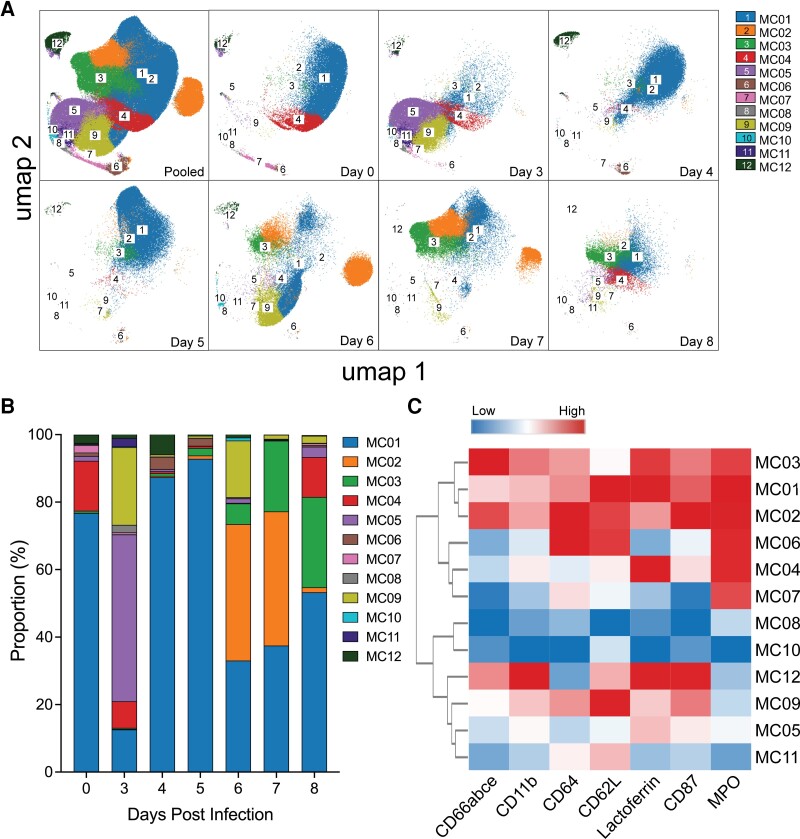
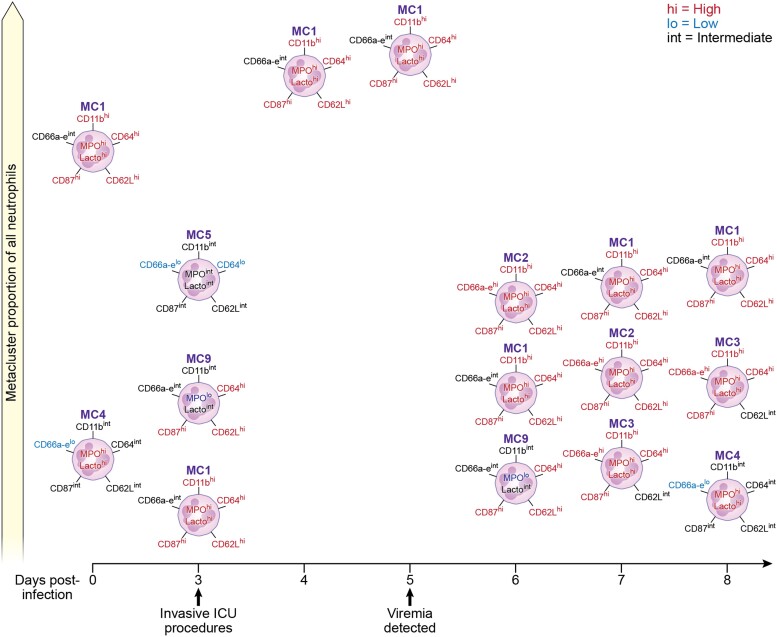
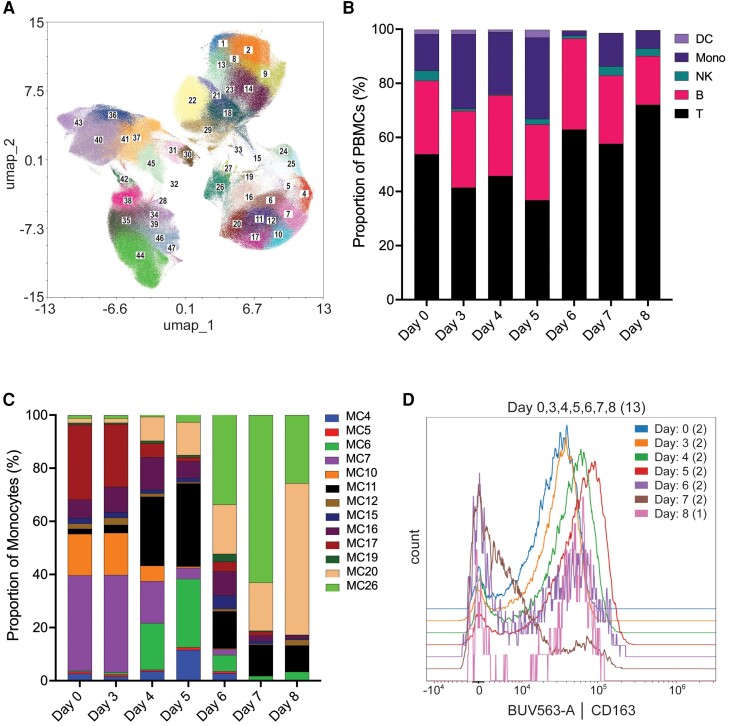
Methods: Two rhesus macaques received a target dose of 1000 plaque-forming units of Ebola virus intramuscularly with supportive care initiated on day 3. High-dimensional spectral cytometry was used to phenotype neutrophils and peripheral blood mononuclear cells daily.
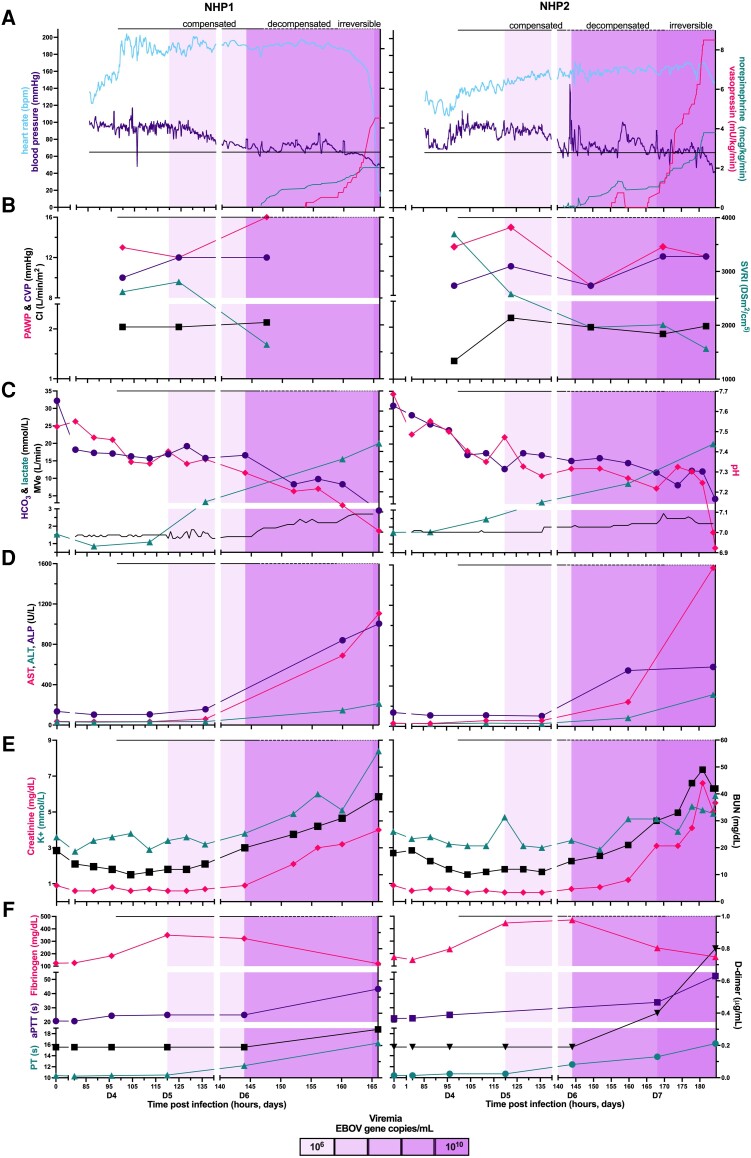
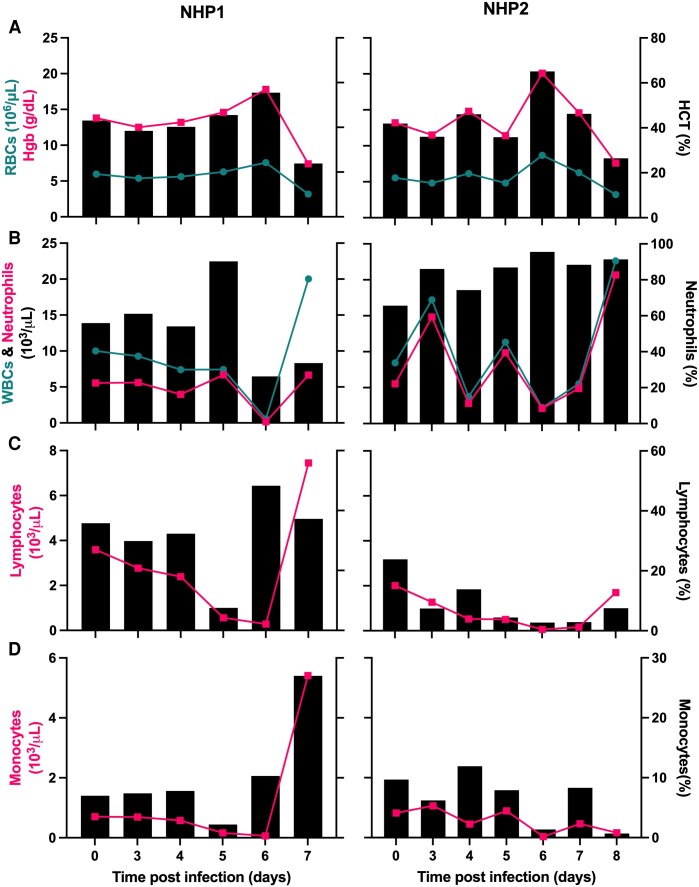
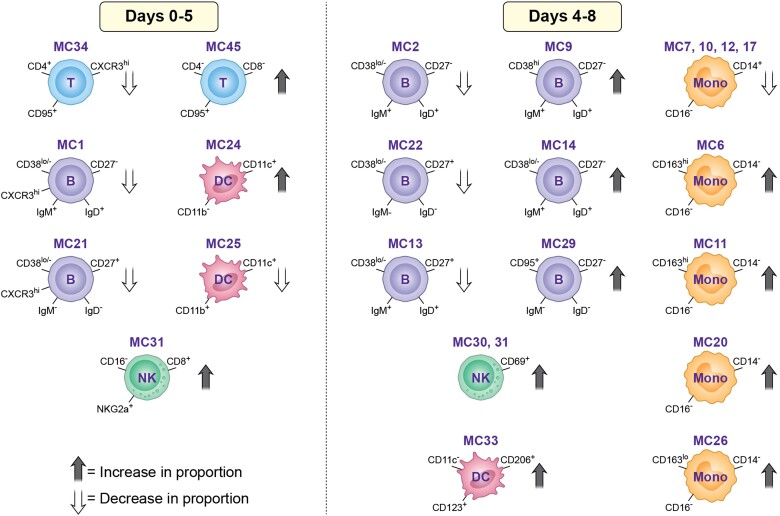
Results: We observed progressive vasodilatory shock with preserved cardiac function following viremia onset on day 5. Multiorgan dysfunction began on day 6 coincident with the nadir of circulating neutrophils. Consumptive coagulopathy and anemia occurred on days 7 to 8 along with irreversible shock, followed by death. The monocyte repertoire began shifting on day 4 with a decline in classical and expansion of double-negative monocytes. A selective loss of CXCR3-positive B and T cells, expansion of naive B cells, and activation of natural killer cells followed viremia onset.
Conclusions: Our model allows for high-fidelity characterization of the pathophysiology of acute Ebola virus infection with host innate and adaptive immune responses, which may advance host-targeted therapy design and evaluation for use after the onset of multiorgan failure.
Keywords: Ebola virus; filovirus; intensive care; nonhuman primate; pathogenesis.
Published by Oxford University Press on behalf of Infectious Diseases Society of America 2023.
Conflict of interest statement
Potential conflicts of interest. All authors: No reported conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Baseler L, Chertow DS, Johnson KM, Feldman H, Morens DM. The pathogenesis of Ebola virus disease. Annu Rev Pathol 2017; 12:387–418. - PubMed
-
- Centers for Disease Control and Prevention [. Accessed 15 May 2023.]. https://www.cdc.gov/vhf/Ebola/history/chronology.html . History of Ebola outbreaks.
-
- Kortepeter MG, Lawler JV, Honko A, et al. . Real-time monitoring of cardiovascular function in rhesus macaques infected with Zaire ebolavirus. J Infect Dis 2011; 204:S1000–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
