

Clinical presentation, outcomes, and threshold for repair by sex in degenerative saccular vs fusiform aneurysms in the descending thoracic aorta
- PMID: 37652142
- PMCID: PMC10841204
- DOI: 10.1016/j.jvs.2023.06.104
Clinical presentation, outcomes, and threshold for repair by sex in degenerative saccular vs fusiform aneurysms in the descending thoracic aorta
Abstract
Objective: Saccular-shaped thoracic aortic aneurysms (TAAs) are often treated at smaller diameters compared with fusiform TAAs, despite a lack of strong clinical evidence to support this practice. The aim of this study was to examine differences in presentation, treatment, and outcomes between saccular TAAs and fusiform TAAs in the descending thoracic aorta. We also examined the need for sex-specific treatment thresholds for TAAs.
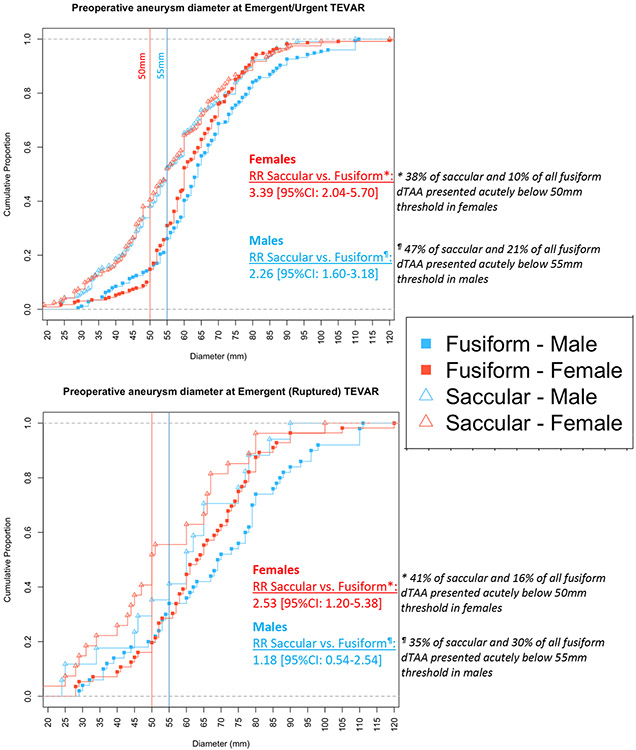
Methods: All Vascular Quality Initiative (VQI) patients undergoing thoracic endovascular aneurysm repair (TEVAR) for degenerative TAAs in the descending thoracic aorta from 2012 through 2022 were reviewed. Patients were stratified by urgency: emergent/urgent vs elective repairs (ruptured/symptomatic). Demographics, comorbidities, anatomical/procedural characteristics, and outcomes for fusiform TAAs and saccular TAAs were compared. Cumulative distribution curves were used to plot the proportion of patients who underwent emergent/urgent repair according to sex-stratified aortic diameter.
Results: Among 655 emergent/urgent TEVARs, 37% were performed for saccular TAAs, whereas among 1352 elective TEVARs, 35% had saccular TAA morphology. Compared with fusiform TAAs, saccular TAAs more frequently underwent emergent/urgent (ruptured/symptomatic) TEVAR below the repair threshold in both females (<50 mm: 38% vs 10%; relative risk, 3.39; 95% confidence interval [CI], 2.04-5.70; P < .001), and males (<55 mm: 47% vs 21%; relative risk, 2.26; 95% CI, 1.60-3.18; P < .001). Moreover, among patients with emergent/urgent fusiform TAAs, females presented at smaller diameters compared with males, whereas there was no difference in preoperative aneurysm diameter among patients with saccular TAAs. Regarding outcomes, emergent/urgent treated saccular TAAs had similar postoperative outcomes and 5-year mortality compared with fusiform TAAs. Nevertheless, in the elective cohort, patients with saccular TAAs had similar postoperative mortality compared with those with fusiform TAAs, but a lower rate of postoperative spinal cord ischemia (0.7% vs 3.2%; P = .010). Furthermore, patients with saccular TAAs had a higher rate of 5-year mortality compared with their fusiform counterparts (23% vs 17%; hazard ratio, 1.53; 95% CI, 1.12-2.10; P = .010).
Conclusions: Patients with saccular TAAs underwent emergent/urgent TEVAR at smaller diameters than those with fusiform TAAs, supporting current clinical practice guideline recommendations that saccular TAAs warrant treatment at smaller diameters. Furthermore, these data support a sex-specific treatment threshold for patients with fusiform TAAs, but not for those with saccular TAAs. Although there were no differences in outcomes following TEVAR between morphologies in the emergent/urgent cohort, patients with saccular TAAs who were treated electively were associated with higher 5-year mortality compared with those with fusiform TAAs.
Keywords: Fusiform; Repair threshold; Saccular; Sex-specific; Thoracic aortic aneurysm.
Copyright © 2023 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures H.V. reports consultant for Medtronic, WL Gore, Terumo, Endologix, and Philips.
Figures

References
-
- Nathan DP, Xu C, Pouch AM, Chandran KB, Desjardins B, Gorman JH, et al. Increased wall stress of saccular versus fusiform aneurysms of the descending thoracic aorta. Annals of Vascular Surgery. 2011;25(8):1129–37. - PubMed
-
- Upchurch GR, Escobar GA, Azizzadeh A, Beck AW, Conrad MF, Matsumura JS, et al. Society for Vascular Surgery clinical practice guidelines of thoracic endovascular aortic repair for descending thoracic aortic aneurysms. Journal of Vascular Surgery. 2021;73(1):55S–83S. - PubMed
-
- Committee W, Riambau V, Böckler D, Brunkwall J, Cao P, Chiesa R, et al. Editor’s Choice – Management of Descending Thoracic Aorta Diseases: Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). European Journal of Vascular and Endovascular Surgery. 2017;53(1):4–52. - PubMed
-
- Isselbacher EM, Preventza O, Black JH, Augoustides JG, Beck AW, Bolen MA, et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Vol. 146, Circulation. 2022. - PMC - PubMed
-
- Karthaus EG, Tong TML, Vahl A, Hamming JF. Saccular Abdominal Aortic Aneurysms: Patient Characteristics, Clinical Presentation, Treatment, and Outcomes in the Netherlands. Annals of Surgery. 2019;270(5). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
