

Predictive performance of automated surveillance algorithms for intravascular catheter bloodstream infections: a systematic review and meta-analysis
- PMID: 37653559
- PMCID: PMC10468855
- DOI: 10.1186/s13756-023-01286-0
Predictive performance of automated surveillance algorithms for intravascular catheter bloodstream infections: a systematic review and meta-analysis
Abstract
Background: Intravascular catheter infections are associated with adverse clinical outcomes. However, a significant proportion of these infections are preventable. Evaluations of the performance of automated surveillance systems for adequate monitoring of central-line associated bloodstream infection (CLABSI) or catheter-related bloodstream infection (CRBSI) are limited.
Objectives: We evaluated the predictive performance of automated algorithms for CLABSI/CRBSI detection, and investigated which parameters included in automated algorithms provide the greatest accuracy for CLABSI/CRBSI detection.
Methods: We performed a meta-analysis based on a systematic search of published studies in PubMed and EMBASE from 1 January 2000 to 31 December 2021. We included studies that evaluated predictive performance of automated surveillance algorithms for CLABSI/CRBSI detection and used manually collected surveillance data as reference. We estimated the pooled sensitivity and specificity of algorithms for accuracy and performed a univariable meta-regression of the different parameters used across algorithms.
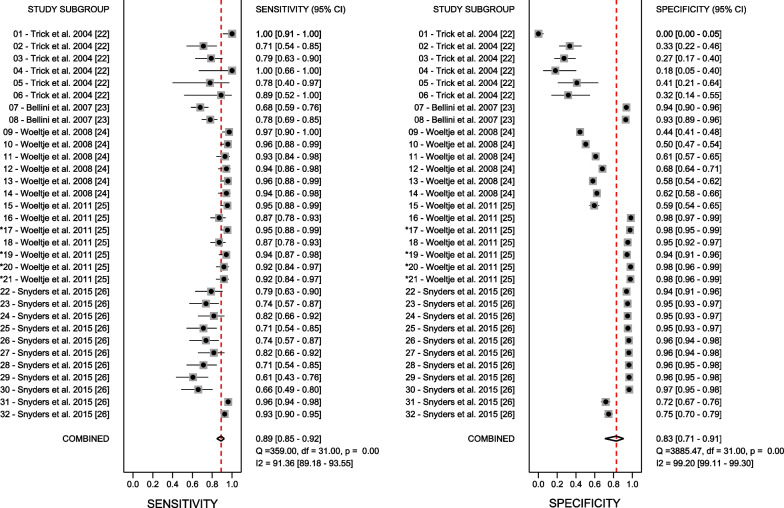
Results: The search identified five full text studies and 32 different algorithms or study populations were included in the meta-analysis. All studies analysed central venous catheters and identified CLABSI or CRBSI as an outcome. Pooled sensitivity and specificity of automated surveillance algorithm were 0.88 [95%CI 0.84-0.91] and 0.86 [95%CI 0.79-0.92] with significant heterogeneity (I2 = 91.9, p < 0.001 and I2 = 99.2, p < 0.001, respectively). In meta-regression, algorithms that include results of microbiological cultures from specific specimens (respiratory, urine and wound) to exclude non-CRBSI had higher specificity estimates (0.92, 95%CI 0.88-0.96) than algorithms that include results of microbiological cultures from any other body sites (0.88, 95% CI 0.81-0.95). The addition of clinical signs as a predictor did not improve performance of these algorithms with similar specificity estimates (0.92, 95%CI 0.88-0.96).
Conclusions: Performance of automated algorithms for detection of intravascular catheter infections in comparison to manual surveillance seems encouraging. The development of automated algorithms should consider the inclusion of results of microbiological cultures from specific specimens to exclude non-CRBSI, while the inclusion of clinical data may not have an added-value. Trail Registration Prospectively registered with International prospective register of systematic reviews (PROSPERO ID CRD42022299641; January 21, 2022). https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022299641.
Keywords: Accuracy; Algorithm; Automated monitoring; CLABSI; CRBSI; Healthcare associated infections; Surveillance.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
PWS received travel grants from Pfizer and Gilead, speaker’s honorary from Pfizer and fees for advisory board activity from Pfizer and Gilead outside of the submitted work. We declare that the authors have no competing interests as defined by BMC, or other interests that might be perceived to influence the results and/or discussion reported in this paper.
Figures


References
-
- Suetens C, Latour K, Kärki T, Ricchizzi E, Kinross P, Moro ML, et al. Healthcare-Associated Infections Prevalence Study Group. Prevalence of healthcare-associated infections estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: results from two European point prevalence surveys, 2016 to 2017. Euro Surveill. 2018;23(46):1800516. Erratum in: Euro Surveill. 2018;23(47). - PMC - PubMed
-
- Zarb P, Coignard B, Griskeviciene J, Muller A, Vankerckhoven V, Weist K, et al. National Contact Points for the ECDC pilot point prevalence survey; Hospital Contact Points for the ECDC pilot point prevalence survey. The european centre for disease prevention and control (ECDC) pilot point prevalence survey of healthcare-associated infections and antimicrobial use. Euro Surveill. 2012;17(46):20316. - PubMed
-
- Schreiber PW, Sax H, Wolfensberger A, Clack L, Kuster SP, Swissnoso. The preventable proportion of healthcare-associated infections 2005–2016: Systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2018;39(11):1277–95. - PubMed
-
- European Centre for Disease Prevention and Control. Healthcare-associated infections in intensive care units - Annual Epidemiological Report for 2017. ECDC; 2019. https://www.ecdc.europa.eu/sites/default/files/documents/AER_for_2017-HA....
