

Lateral Ankle Instability after Rotational Injury: A Case Report
- PMID: 37654758
- PMCID: PMC10465758
- DOI: 10.13107/jocr.2023.v13.i08.3848
Lateral Ankle Instability after Rotational Injury: A Case Report
Abstract
Introduction: One of the most common orthopedic injury injuries seen in patients at the emergency department is that of the ankle. There are some efficient protocols for their treatment, but more often the clinician is fo-cused in finding and treating possible fractures and disregards ligamentous lesions that lead to instabil-ity, if they become chronic.
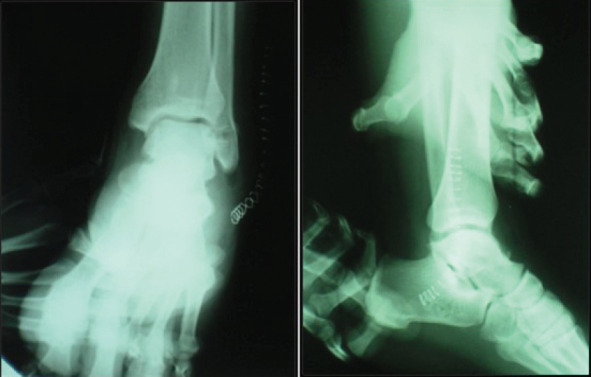
Case report: A patient that suffered an ankle sprain was improperly handled, developed lateral instability of the ankle, and was treated surgically using an autologous semitendinosus graft. A 42-year year-old Caucasian male that after an ankle sprain was examined in various primary health -care centers, four times within six 6 months, with persistent symptoms of his left ankle. After all these months, he was eventually diagnosed with post-traumatic lateral instability of the ankle that was resistant to con-servative treatment. In stress view X-rays, the talar tilt angle was 21°ο and the anterior drawer was measured at 13 mm. The patient was treated surgically with reconstruction of the anterior talofibular and the calcaneofibular ligament using an autologous semitendinosus graft from the left knee. The graft was pinned in the anatomical insertion sites of the ligaments with absorbable screws. A post-surgical physiotherapy regimen was applied for two 2 months. In the post-surgical dynamic stress view X-rays, the talar tilt angle and the anterior drawer were markedly improved, measured at 3°ο and 4 mm, respec-tively. In 11 months post-surgical follow-up, the patient's American Foot and Ankle Score was 85, from the 60 evaluated before treatment.
Conclusion: The use of guidelines, regular follow-ups, and functional rehabilitation are key factors to treating ankle injuries. The reconstruction of lateral collateral ligament complex with a semitendinosus graft is one of the surgical options for restoring lateral ankle instability.
Keywords: Ankle sprain; autologous semitendinosus graft; lateral instability of the ankle.
Copyright: © Indian Orthopaedic Research Group.
Conflict of interest statement
Conflict of Interest: Nil
Figures








Similar articles
-
[Reconstruction of anterior talofibular ligament and calcaneofibular ligament with autologous peroneus brevis tendon in the treatment of chronic lateral ankle instability].Zhongguo Gu Shang. 2022 Feb 25;35(2):172-7. doi: 10.12200/j.issn.1003-0034.2022.02.016. Zhongguo Gu Shang. 2022. PMID: 35191272 Chinese.
-
Comparison Between the Simultaneous Reconstructions of the Anterior Talofibular Ligament and Calcaneofibular Ligament and the Single Reconstruction of the Anterior Talofibular Ligament for the Treatment of Chronic Lateral Ankle Instability.J Foot Ankle Surg. 2022 May-Jun;61(3):533-536. doi: 10.1053/j.jfas.2021.01.012. Epub 2021 Oct 22. J Foot Ankle Surg. 2022. PMID: 34785128
-
Anatomic reconstruction of the anterior talofibular and calcaneofibular ligaments using a semitendinosus tendon allograft and interference screws.Knee Surg Sports Traumatol Arthrosc. 2012 Aug;20(8):1432-7. doi: 10.1007/s00167-011-1666-y. Epub 2011 Sep 21. Knee Surg Sports Traumatol Arthrosc. 2012. PMID: 21935617
-
A Rare Pattern of Ligamentous Injury of the Ankle: A Case Report and Review of the Literature.J Foot Ankle Surg. 2021 Jul-Aug;60(4):870-872. doi: 10.1053/j.jfas.2021.03.001. Epub 2021 Mar 6. J Foot Ankle Surg. 2021. PMID: 33820682 Review.
-
Treatment of acute lateral ankle ligament rupture in the athlete. Conservative versus surgical treatment.Sports Med. 1999 Jan;27(1):61-71. doi: 10.2165/00007256-199927010-00005. Sports Med. 1999. PMID: 10028133 Review.
References
-
- Trevino SG, Davis P, Hecht PJ. Management of acute and chronic lateral ligament injuries of the ankle. Orthop Clin North Am. 1994;25:1–16. - PubMed
-
- Struijs P, Kerkhoffs G. Ankle sprain. Clin Evid. 2006;15:1493–501. - PubMed
-
- Peters JW, Trevino SG, Renstrom PA. Chronic lateral ankle instability. Foot Ankle. 1991;12:182–91. - PubMed
-
- Groff GD. Ankle sprain. In: Klippel J, Dieppe P, editors. Rheumatology. Vol. 14. London: Mosby; 1998. pp. 10–14.13.
Publication types
LinkOut - more resources
Full Text Sources