

Arthroscopic Labral Repair and Pancapsular Shift With Knotless All-Suture Anchors in the Setting of Multidirectional Instability of the Shoulder
- PMID: 37654880
- PMCID: PMC10466139
- DOI: 10.1016/j.eats.2023.03.020
Arthroscopic Labral Repair and Pancapsular Shift With Knotless All-Suture Anchors in the Setting of Multidirectional Instability of the Shoulder
Abstract
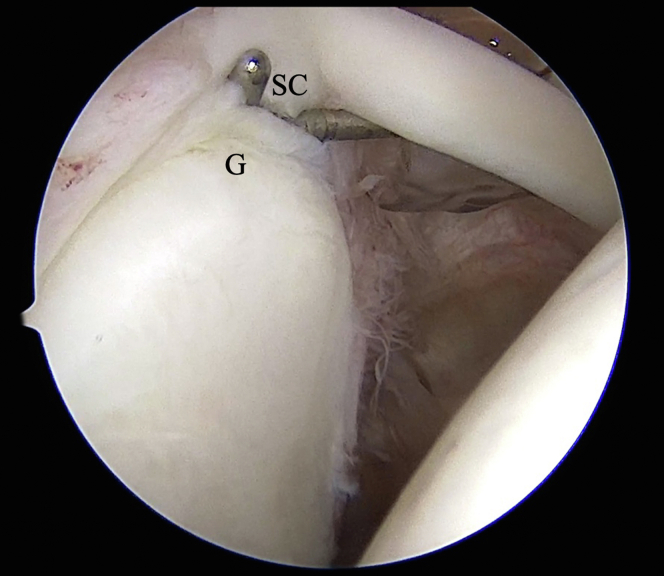
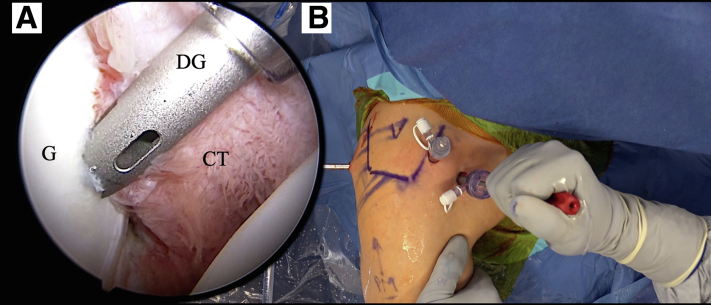
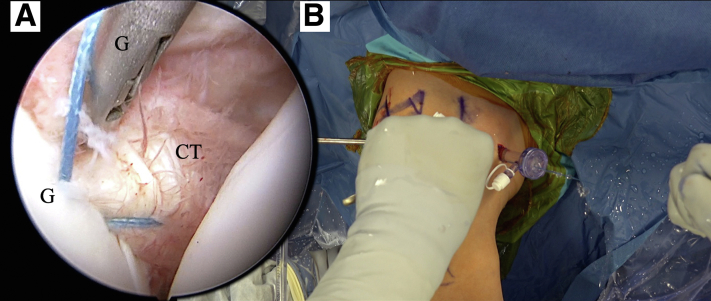
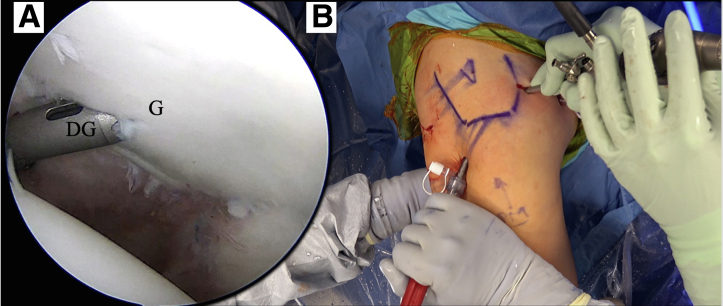
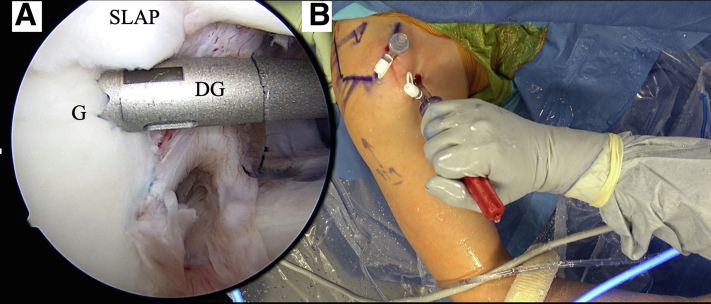
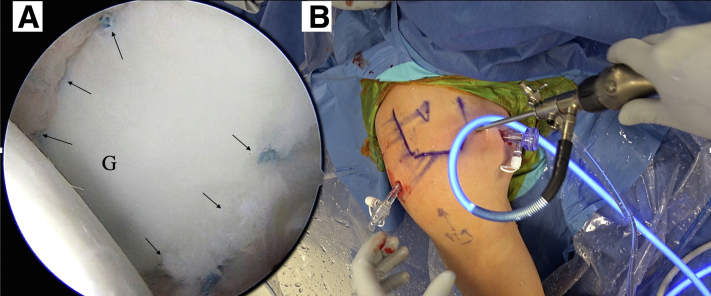
In the management of multidirectional type of shoulder instability (MDI), arthroscopic surgical stabilization is a preferred treatment option after failed conservative therapy regimens because of the ability to easily access all aspects of the capsule with one surgical procedure. As arthroscopic techniques have evolved, factors critical to postoperative success have been elucidated. Currently, optimal arthroscopic treatment of MDI involves circumferentially restoring labral integrity, a tailored, patient-specific surgical reduction of capsular volume, and adequately managing potential lesions of the biceps anchor. The purpose of this article and accompanying video is to present our technique for arthroscopic circumferential labral repair and pancapsular shift using knotless all-suture anchors in the setting of MDI with a concurrent type II SLAP lesion.
© 2023 Published by Elsevier Inc. on behalf of the Arthroscopy Association of North America.
Figures
Similar articles
-
Arthroscopic Pancapsular Shift With Labral Repair for Multidirectional Instability of the Shoulder.Arthrosc Tech. 2017 Jul 24;6(4):e1113-e1117. doi: 10.1016/j.eats.2017.03.032. eCollection 2017 Aug. Arthrosc Tech. 2017. PMID: 29354405 Free PMC article.
-
Complications and Return to Activity After Arthroscopic Repair of Isolated Type II SLAP Lesions: A Systematic Review Comparing Knotted Versus Knotless Suture Anchors.Orthop J Sports Med. 2020 Apr 20;8(4):2325967120911361. doi: 10.1177/2325967120911361. eCollection 2020 Apr. Orthop J Sports Med. 2020. PMID: 32341926 Free PMC article. Review.
-
Outcomes After Arthroscopic Pancapsular Capsulorrhaphy With Suture Anchors for the Treatment of Multidirectional Glenohumeral Instability in Athletes.Am J Sports Med. 2016 Dec;44(12):3188-3197. doi: 10.1177/0363546516659644. Epub 2016 Aug 19. Am J Sports Med. 2016. PMID: 27543145
-
Knotless PEEK and double-loaded biodegradable suture anchors ensure comparable clinical outcomes in the arthroscopic treatment of traumatic anterior shoulder instability: a prospective randomized study.Knee Surg Sports Traumatol Arthrosc. 2022 Nov;30(11):3835-3841. doi: 10.1007/s00167-022-06969-6. Epub 2022 Apr 18. Knee Surg Sports Traumatol Arthrosc. 2022. PMID: 35435470 Free PMC article. Clinical Trial.
-
Knotted Versus Knotless Anchors for Labral Repair in the Shoulder: A Systematic Review.Arthroscopy. 2021 Apr;37(4):1314-1321. doi: 10.1016/j.arthro.2020.11.056. Epub 2020 Dec 9. Arthroscopy. 2021. PMID: 33307150
Cited by
-
Two-Portal Arthroscopic Knotless All-Suture Anchor Posterior Labral Repair.Arthrosc Tech. 2024 Feb 11;13(5):102928. doi: 10.1016/j.eats.2024.102928. eCollection 2024 May. Arthrosc Tech. 2024. PMID: 38835471 Free PMC article.
-
Outcomes After Arthroscopic Posterior Labral Repair With All-Suture Anchors in Football Players.Orthop J Sports Med. 2025 Jun 11;13(6):23259671251343646. doi: 10.1177/23259671251343646. eCollection 2025 Jun. Orthop J Sports Med. 2025. PMID: 40519542 Free PMC article.
References
-
- Longo U.G., Rizzello G., Loppini M., et al. Multidirectional instability of the shoulder: A systematic review. Arthroscopy. 2015;31:2431–2443. - PubMed
-
- Neer C.S., 2nd Involuntary inferior and multidirectional instability of the shoulder: Etiology, recognition, and treatment. Instr Course Lect. 1985;34:232–238. - PubMed
-
- Gerber C., Nyffeler R.W. Classification of glenohumeral joint instability. Clin Orthop Relat Res. 2002;400:65–76. - PubMed
-
- Kraeutler M.J., McCarty E.C., Belk J.W., et al. Descriptive Epidemiology of the MOON Shoulder Instability Cohort. Am J Sports Med. 2018;46:1064–1069. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
