

Clinical and MRI Outcomes of Repaired Peripheral Longitudinal Tears of the Posterior Horn of the Medial Meniscus With ACL Reconstruction: Results According to Tear Size
- PMID: 37655242
- PMCID: PMC10467388
- DOI: 10.1177/23259671231167535
Clinical and MRI Outcomes of Repaired Peripheral Longitudinal Tears of the Posterior Horn of the Medial Meniscus With ACL Reconstruction: Results According to Tear Size
Abstract
Background: Arthroscopic repair of longitudinal tears in the medial meniscal posterior horn (MMPH) has been reported to result in high rates of meniscal healing when performed alongside anterior cruciate ligament reconstruction (ACLR). However, studies that have focused on longitudinal tears and their impact on clinical outcomes after arthroscopic repair are insufficient.
Purpose: To investigate the clinical outcome and healing status after concomitant arthroscopic ACLR and repair of MMPH peripheral longitudinal tears, with respect to the tear length.
Study design: Cohort study; Level of evidence, 3.
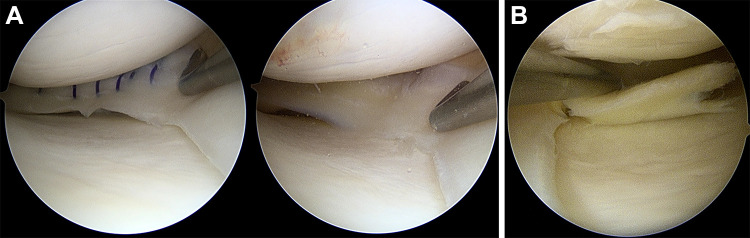
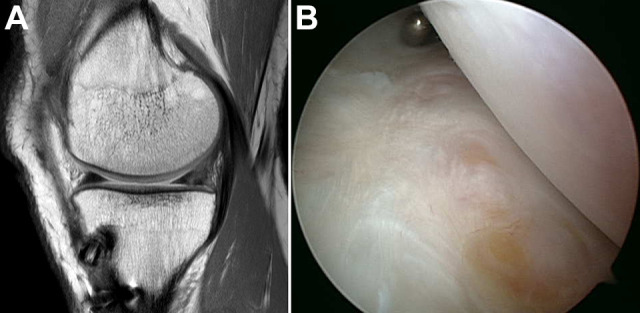
Methods: A total of 263 patients who underwent concurrent arthroscopic suture repair of longitudinal tears of the MMPH and ACLR were enrolled. All patients had 2-year postoperative magnetic resonance imaging (MRI) evaluations, and 61% of patients underwent a second-look arthroscopy. The exclusion criteria were partial meniscectomies and multiligament injuries. Patients were assessed pre- and postoperatively for clinical scores, amount of anterior translation, grade of pivot shift, and presence of meniscal tear extension. According to the length of longitudinal tears, patients were classified into 2 groups: (1) patients with tears that were located in the posterior compartment and (2) patients with tears that extended to the midbody of the meniscus. Binary stepwise logistic regression analysis was used to evaluate the risk factors for unhealed menisci as identified by MRI.
Results: A total of 83 patients were included in this study-52 patients (group 1) had MMPH tears without tear extension and 31 patients (group 2) had MMPH tears with tear extension. There were no differences in outcomes between the groups, including the healing rate after meniscal repair (P > .05). Based on postoperative MRI scans, 67 patients (80.7%) were categorized as completely healed and 16 patients (19.3%) as unhealed. There were no significant differences between the completely healed and unhealed groups in outcomes or the rate of preoperative midbody tear extension. Higher body mass index and lower preoperative Lysholm scores were identified as risk factors for unhealed menisci.
Conclusion: Overall, the rate of complete healing of MMPH tears repaired concomitantly with ACLR was 80.7% (67/83), and midbody tear extension did not affect the healing rate of the repaired meniscus. Results indicate that suture repair for unstable MMPH tears should be considered regardless of tear size.
Keywords: anterior cruciate ligament; magnetic resonance imaging; medial meniscal posterior horn; meniscal repair; peripheral longitudinal tear of medial meniscus.
© The Author(s) 2023.
Conflict of interest statement
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Acosta J, Ravaei S, Brown SM, Mulcahey MK. Examining techniques for treatment of medial meniscal ramp lesions during anterior cruciate ligament reconstruction: a systematic review. Arthroscopy. 2020;36(11):2921–2933. - PubMed
-
- Ahn JH, Lee YS, Yoo JC, et al. Clinical and second-look arthroscopic evaluation of repaired medial meniscus in anterior cruciate ligament-reconstructed knees. Am J Sports Med. 2010;38(3):472–477. - PubMed
-
- Ahn JH, Yoo JC, Lee SH. Posterior horn tears: all-inside suture repair. Clin Sports Med. 2012;31(1):113–134. - PubMed
-
- Albayrak K, Buyukkuscu MO, Kurk MB, et al. Leaving the stable ramp lesion unrepaired does not negatively affect clinical and functional outcomes as well as return to sports rates after ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2021;29(11):3773–3781. - PubMed
-
- Alessio-Mazzola M, Lovisolo S, Capello AG, et al. Management of ramp lesions of the knee: a systematic review of the literature. Musculoskelet Surg. 2020;104(2):125–133. - PubMed
LinkOut - more resources
Full Text Sources
