

Arthroscopic Biological Augmentation With Subacromial Bursa for Bursal-Sided Partial-Thickness Rotator Cuff Tears
- PMID: 37655250
- PMCID: PMC10467416
- DOI: 10.1177/23259671231190335
Arthroscopic Biological Augmentation With Subacromial Bursa for Bursal-Sided Partial-Thickness Rotator Cuff Tears
Abstract
Background: Augmentation with subacromial bursa has not been fully established in bursal-sided partial-thickness rotator cuff tears (PT-RCTs).
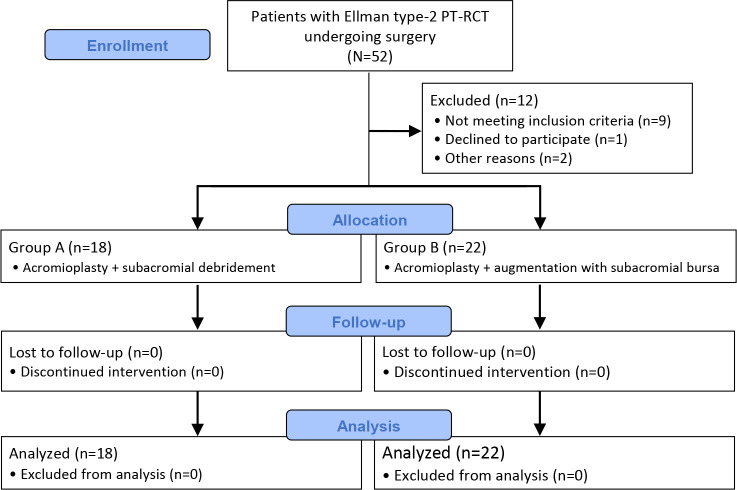
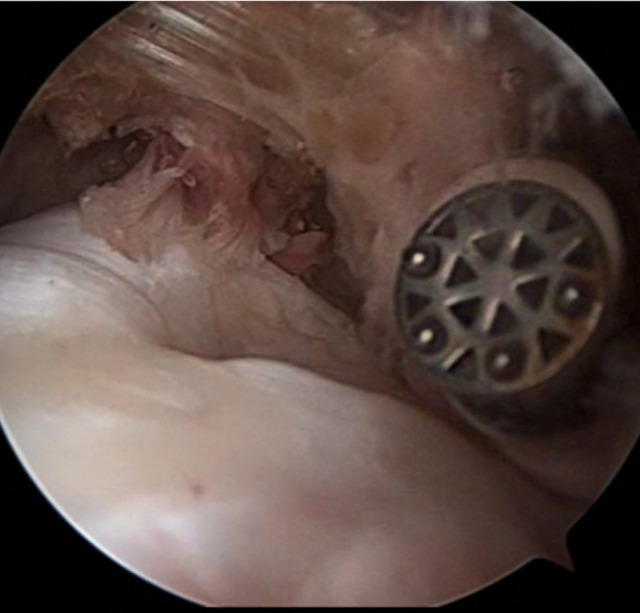
Purpose: To compare the results of acromioplasty + arthroscopic debridement versus acromioplasty + augmentation with subacromial bursa for Ellman type 2 PT-RCTs involving 25% to 50% of the tendon surface area.
Study design: Cohort study; Level of evidence, 3.
Methods: Included were 40 patients (mean age, 47.8 years) with Ellman type 2 PT-RCTs whose symptoms did not regress despite 3 months of nonoperative treatment. The patients underwent either acromioplasty + debridement (group A; n = 18) or acromioplasty + augmentation (group B; n = 22). Outcome scores (visual analog scale [VAS] pain score, Constant-Murley score [CMS], and American Shoulder and Elbow Surgeons [ASES] score) were obtained preoperatively and at 6, 12, and 18 months postoperatively. Magnetic resonance imaging (MRI) scans performed at 6 months postoperatively were used to determine the integrity and state of healing.
Results: There were no significant differences between groups A and B in preoperative VAS, CMS, or ASES scores, and patients in both groups saw significant improvement at each follow-up time point on all 3 outcome scores (P = .001 for all). Scores on all 3 outcome measures were significantly better in group B than group A at each postoperative time point (P < .05 for all). Postoperative MRI scans revealed persistent partial tears in 5 of 18 patients in group A compared with 2 of 22 patients in group B (P < .05). Conversion to full-thickness tear (3/18 patients) was seen only in group A.
Conclusion: Patients who underwent biological augmentation of their PT-RCTs had improved outcome scores compared with those treated with acromioplasty and debridement alone.
Keywords: bursal side; full thickness; partial thickness; rotator cuff; subacromial bursa.
© The Author(s) 2023.
Conflict of interest statement
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures



Similar articles
-
Comparison of Arthroscopic Debridement and Repair in the Treatment of Ellman Grade II Bursal-side Partial-thickness Rotator Cuff Tears: A Prospective Randomized Controlled Trial.Orthop Surg. 2021 Oct;13(7):2070-2080. doi: 10.1111/os.13130. Epub 2021 Oct 1. Orthop Surg. 2021. PMID: 34596965 Free PMC article. Clinical Trial.
-
A comparative study of arthroscopic débridement versus repair for Ellman grade II bursal-side partial-thickness rotator cuff tears.J Shoulder Elbow Surg. 2020 Oct;29(10):2072-2079. doi: 10.1016/j.jse.2020.03.006. Epub 2020 Jun 1. J Shoulder Elbow Surg. 2020. PMID: 32499197
-
Short-term Outcomes of Arthroscopic Debridement and Selected Acromioplasty of Bursal- vs Articular-Sided Partial-Thickness Rotator Cuff Tears of Less Than 50.Orthop J Sports Med. 2018 Aug 27;6(8):2325967118792001. doi: 10.1177/2325967118792001. eCollection 2018 Aug. Orthop J Sports Med. 2018. PMID: 30182028 Free PMC article.
-
Surgery for rotator cuff tears.Cochrane Database Syst Rev. 2019 Dec 9;12(12):CD013502. doi: 10.1002/14651858.CD013502. Cochrane Database Syst Rev. 2019. PMID: 31813166 Free PMC article.
-
A systematic review of randomized control trials looking at functional improvement of rotator cuff partial thickness tears following platelet-rich-plasma injection: a comparison of glenohumeral joint vs. subacromial bursa vs. intratendinous injection locations.JSES Int. 2024 Jan 24;8(3):464-471. doi: 10.1016/j.jseint.2024.01.003. eCollection 2024 May. JSES Int. 2024. PMID: 38707549 Free PMC article. Review.
Cited by
-
Mini-open transosseous repair with bursal augmentation improves outcomes in massive rotator cuff tears.Sci Rep. 2025 Jan 17;15(1):2333. doi: 10.1038/s41598-025-85520-2. Sci Rep. 2025. PMID: 39824871 Free PMC article.
-
The Evolution of Arthroscopic Shoulder Surgery: Current Trends and Future Perspectives.J Clin Med. 2025 Apr 1;14(7):2405. doi: 10.3390/jcm14072405. J Clin Med. 2025. PMID: 40217855 Free PMC article. Review.
References
-
- Chung SW, Kim JY, Yoon JP, Lyu SH, Rhee SM, Oh SB. Arthroscopic repair of partial-thickness and small full-thickness rotator cuff tears: tendon quality as a prognostic factor for repair integrity. Am J Sports Med. 2015;43(3):588–596. - PubMed
-
- Crisan M, Yap S, Casteilla L, et al. A perivascular origin for mesenchymal stem cells in multiple human organs. Cell Stem Cell. 2008;3(3):301–313. - PubMed
LinkOut - more resources
Full Text Sources
