

The Diagnosis and Treatment of Ampullary Carcinoma
- PMID: 37656482
- PMCID: PMC10714289
- DOI: 10.3238/arztebl.m2023.0195
The Diagnosis and Treatment of Ampullary Carcinoma
Abstract
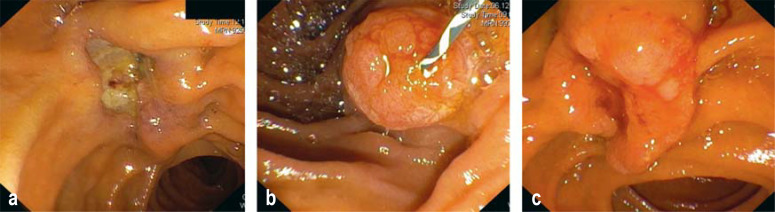
Background: Ampullary or papillary carcinoma is a malignant tumor arising from the mucosa in the region of the major duodenal papilla, also known as the ampulla of Vater. Uniform treatment recommendations are lacking both for the adjuvant situation and for palliative care.
Methods: A selective literature search was carried out in PubMed in order to identify the most informative publications concerning the epidemiology, clinico-pathological background, and surgical and medical treatment of this condition.
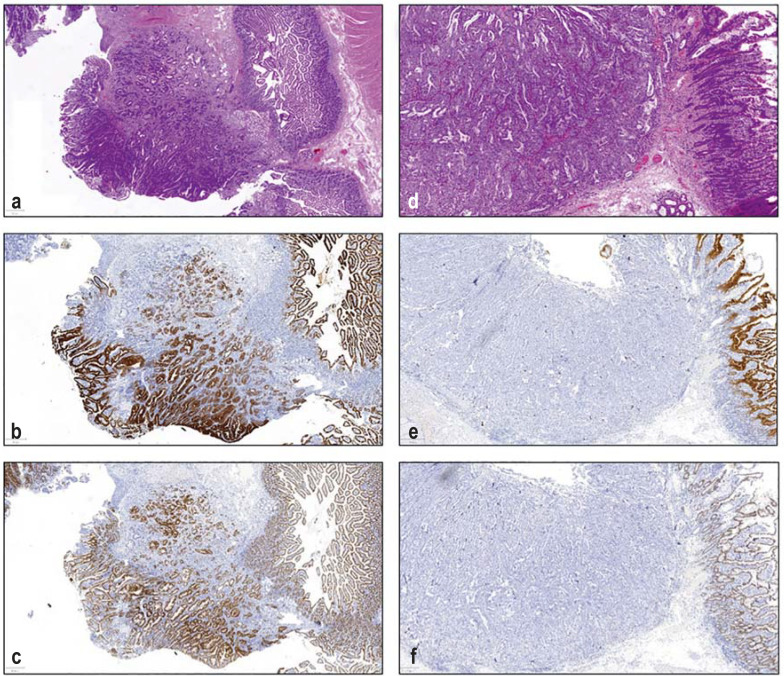
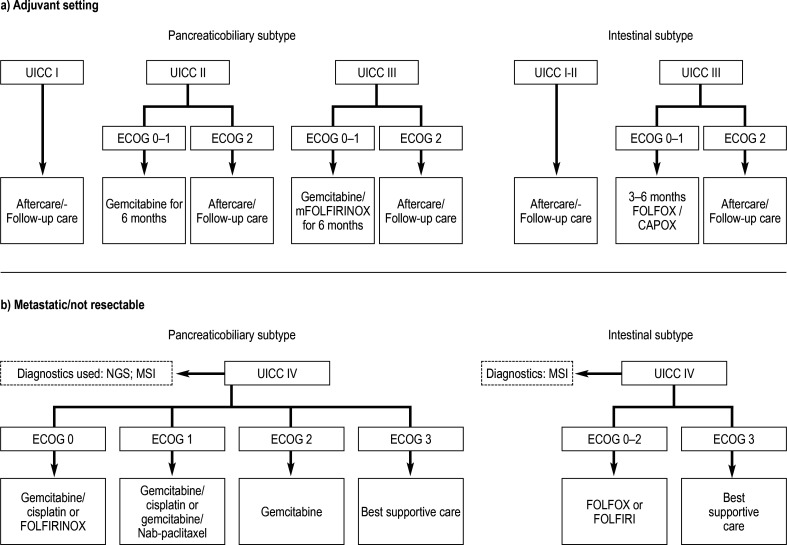
Results: Ampullary carcinoma has an incidence of 0.5 to 0.9 per 100 000 persons and a poor prognosis, with a 5-year survival rate of 41% to 45% for locally confined and 4% to 7% for metastatic disease. Most such tumors are of an intestinal or a pan - creaticobiliary immunohistochemical subtype; the latter has a worse prognosis (median survival, 72-80 vs. 33-41 months). Targeted treatment is not yet available for either subtype, nor is there enough scientific evidence available for the formulation of specific therapeutic recommendations in either the adjuvant or the palliative situation. The treatment of choice for ampullary carcinoma is radical oncological resection of the head of the pancreas with systematic lymphadenectomy. Five-year overall survival is between 10% and 75% depending on the stage. No definitive recommendation for adjuvant therapy can be given. Palliative therapy can be oriented to the published treatment strategies for cancer of the colon, pancreas, and bile duct.
Conclusion: The current state of the evidence on the treatment of ampullary carcinoma is poor. Therapeutic decisions should be discussed in an interdisciplinary tumor board and should, in our opinion, take the histological subtype into account.
Figures
Similar articles
-
[Results of surgical treatment in ampullary and pancreatic carcinoma and its prognostic parameters after R0-resection].Zentralbl Chir. 2005 Aug;130(4):353-61. doi: 10.1055/s-2005-836794. Zentralbl Chir. 2005. PMID: 16103961 German.
-
[Ampullary Carcinoma-prognostic and Therapeutical Contrast to Pancreatic Ductal Adenocarcinoma].Zentralbl Chir. 2022 Apr;147(2):160-167. doi: 10.1055/a-1775-9024. Epub 2022 Apr 4. Zentralbl Chir. 2022. PMID: 35378556 German.
-
Treatment Approach to Adenocarcinoma of the Ampulla of Vater.Curr Treat Options Oncol. 2021 Sep 29;22(11):103. doi: 10.1007/s11864-021-00894-5. Curr Treat Options Oncol. 2021. PMID: 34586537 Review.
-
Role of Adjuvant Multimodality Therapy After Curative-Intent Resection of Ampullary Carcinoma.JAMA Surg. 2019 Aug 1;154(8):706-714. doi: 10.1001/jamasurg.2019.1170. JAMA Surg. 2019. PMID: 31141112 Free PMC article.
-
[Treatment of Ampullary Adenocarcinoma].Korean J Gastroenterol. 2023 Oct 25;82(4):159-170. doi: 10.4166/kjg.2023.110. Korean J Gastroenterol. 2023. PMID: 37876255 Review. Korean.
Cited by
-
Ivory Vertebra Phenomenon as a Sign of Metastatic Dissemination in Pancreatobiliary Neoplasia: A Case Report and Literature Review.Cureus. 2025 Jan 25;17(1):e77978. doi: 10.7759/cureus.77978. eCollection 2025 Jan. Cureus. 2025. PMID: 39872917 Free PMC article.
-
AGR2: The Covert Driver and New Dawn of Hepatobiliary and Pancreatic Cancer Treatment.Biomolecules. 2024 Jun 23;14(7):743. doi: 10.3390/biom14070743. Biomolecules. 2024. PMID: 39062458 Free PMC article. Review.
-
Thioredoxin System Protein Expression in Carcinomas of the Pancreas, Distal Bile Duct, and Ampulla in the United Kingdom.Diseases. 2024 Sep 24;12(10):227. doi: 10.3390/diseases12100227. Diseases. 2024. PMID: 39452470 Free PMC article.
-
Nomogram for overall survival in ampullary adenocarcinoma using the surveillance, epidemiology, and end results database and external validation.World J Clin Oncol. 2025 Feb 24;16(2):95910. doi: 10.5306/wjco.v16.i2.95910. World J Clin Oncol. 2025. PMID: 39995566 Free PMC article.
References
-
- Kaatsch P, Spix C, Katalinic A, Hentschel S, Luttmann S, Stegmaier C. Krebs in Deutschland 2013/2014. In: Robert Koch-Institut; die Gesellschaft der epidemiologischen Krebsregister in Deutschland e.V., editor. 11th edition. Berlin: 2017. www.krebsdaten.de/Krebs/DE/Content/Publikationen/Krebs_in_Deutschland/ki... (last accessed on 1 November 2022)
-
- Albores-Saavedra J, Schwartz AM, Batich K, Henson DE. Cancers of the ampulla of vater: demographics, morphology, and survival based on 5,625 cases from the SEER program. J Surg Oncol. 2009;100:598–605. - PubMed
-
- Sommerville CAM, Limongelli P, Pai M, et al. Survival analysis after pancreatic resection for ampullary and pancreatic head carcinoma: an analysis of clinicopathological factors. J Surg Oncol. 2009;100:651–656. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical