

Socio-economic differences among low-birthweight infants in Hungary. Results of the Cohort '18 -Growing Up in Hungary birth cohort study
- PMID: 37656714
- PMCID: PMC10473525
- DOI: 10.1371/journal.pone.0291117
Socio-economic differences among low-birthweight infants in Hungary. Results of the Cohort '18 -Growing Up in Hungary birth cohort study
Abstract
Background: As Hungary had the fifth-highest rate of low-birthweight (LBW) in the EU27 in 2020, LBW still remains a public health problem for the country.
Objective: Our goal is to examine whether LBW in Hungary is determined by the mothers' educational attainment, adjusted for other maternal characteristics (SES, health behaviour and psychological status during pregnancy) among mothers who gave birth in 2018-2019 in Hungary.
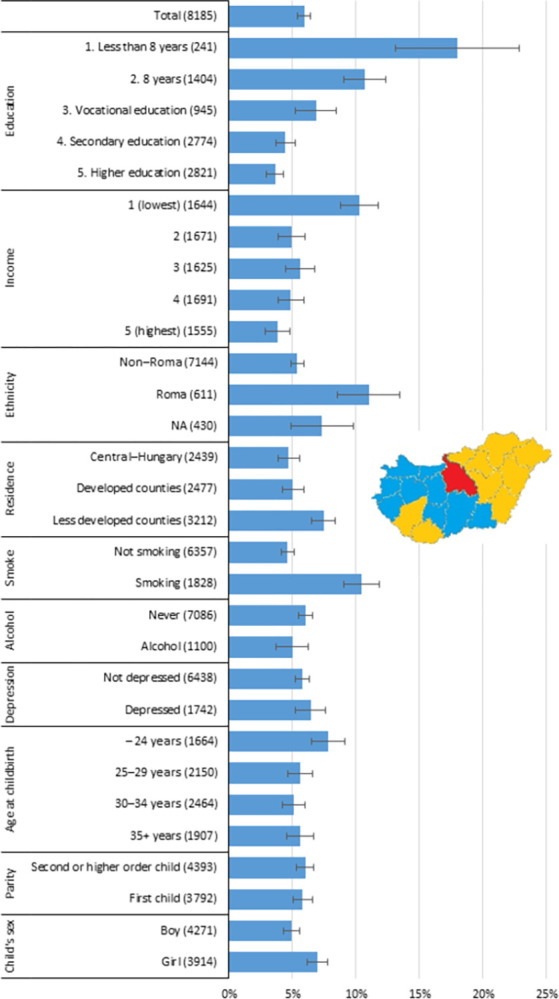
Methods: Source of data is the first and second wave of the Cohort '18 -Growing Up in Hungary longitudinal birth cohort study (n = 8185). It is based on a nationwide representative sample of pregnant women who gave birth between March 2018 and April 2019. All data were self-reported by mothers. We examined the association between maternal educational attainment and the risk of giving birth to an LBW-child (<2500g) by using logistic regression analysis. The highest educational attainment of the mother is measured by a five-value categorical variable (ISCED 97: 0-1; 2; 3C; 3-4; 5-6).
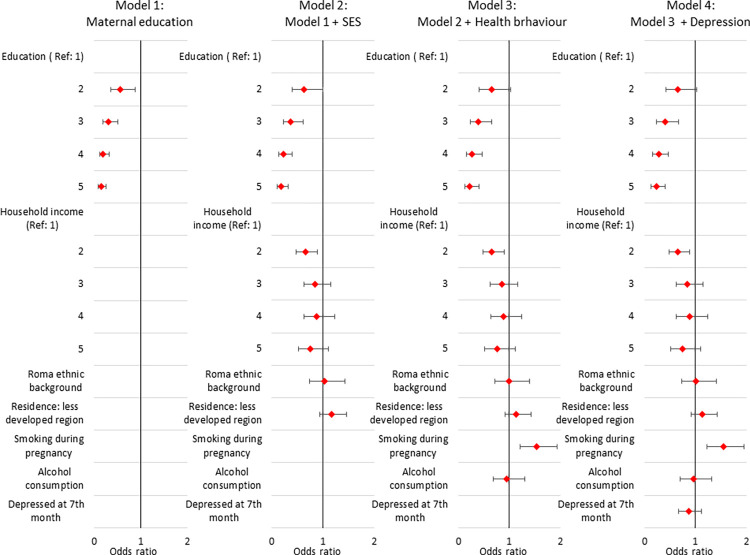
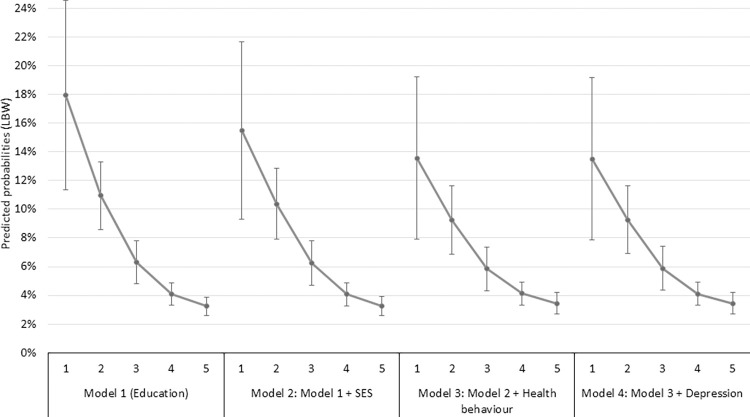
Results: 5.9% of women had LBW children. This rate is 18.0% among the lowest educated women with ISCED 97: 0-1; and it is 3.6% among the highest educated women with ISCED 97: 5-6. The adjusted predicted probabilities of LBW for these two groups of women are 13.5%, and 3.4% respectively, adjusted for household income quantiles, Roma ethnic background, residence place, smoking, alcohol consumption, and depression during pregnancy; controlled for mother's height, age at birth, parity and child's sex. Compared to women with the lowest level of education, the risk of giving birth to an LBW child decreases by 34.6% for those with the second level of education, by 60.1% for those with the third level of education, by 72.5% for those with the fourth level of education and by 77.2% for those with the highest level of education. Smoking during pregnancy significantly increases the risk of giving birth to an LBW by 54.9%. Being depressed at 7th month of pregnancy decreased the risk of giving birth to an LBW child in our sample by 13.2%, however the relationship is not significant.
Conclusion: Our analysis confirmed that maternal educational attainment has a significant impact on the risk of LBW net of by other maternal SES and health behaviour factors. Nevertheless, even after adjusting for these covariates, inequality in LBW by maternal educational attainment persists.
Copyright: © 2023 Szabó, Boros. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. Comprehensive implementation plan on maternal, infant and young child nutrition (No. WHO/NMH/NHD/14.1). 2014. Available from: https://apps.who.int/iris/bitstream/handle/10665/113048/WHO_NMH_NHD_14.1... - PMC - PubMed
-
- Kramer M.S., Victora C.G. Low birth weight and perinatal mortality. In: Semba R.D. and Bloem M.W. (eds), Nutrition and Health in Developing Countries. Nutrition and Health Series. Humana Press, Totowa, NJ. 2001.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
