

Short dual antiplatelet therapy duration after percutaneous coronary intervention in high bleeding risk patients: Systematic review and meta-analysis
- PMID: 37656721
- PMCID: PMC10473507
- DOI: 10.1371/journal.pone.0291061
Short dual antiplatelet therapy duration after percutaneous coronary intervention in high bleeding risk patients: Systematic review and meta-analysis
Abstract
Introduction: Dual antiplatelet therapy (DAPT) following percutaneous coronary intervention (PCI) reduces major adverse cardiovascular events (MACE) and stent thrombosis. However, DAPT duration is a concern in high bleeding risk (HBR) patients. We evaluated the effect of short DAPT (1-3 months) compared to standard DAPT (6-12 months) on bleeding and ischemic events in HBR PCI.
Methods: We searched MEDLINE, Embase and CENTRAL up to August 18, 2022. Randomized controlled trials (RCTs) comparing short DAPT (1-3 months) versus standard DAPT in HBR PCI were included. We assessed risk of bias (RoB) using the Cochrane RoB2 tool, and certainty of evidence using GRADE criteria. Outcomes included MACE, all-cause death, stent thrombosis, major bleeding, and the composite of major or clinically-relevant non-major bleeding. We estimated risk ratios (RR) and 95% confidence intervals (CI) using a random-effects model.
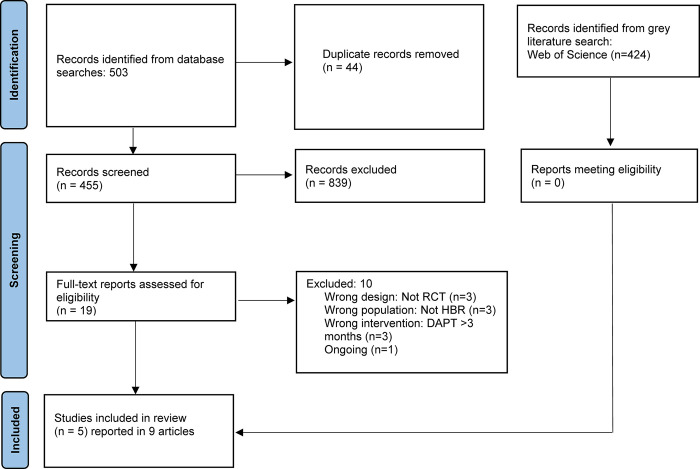
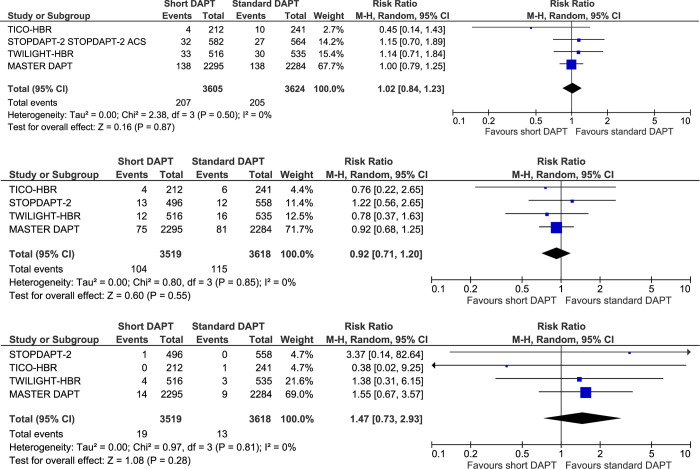
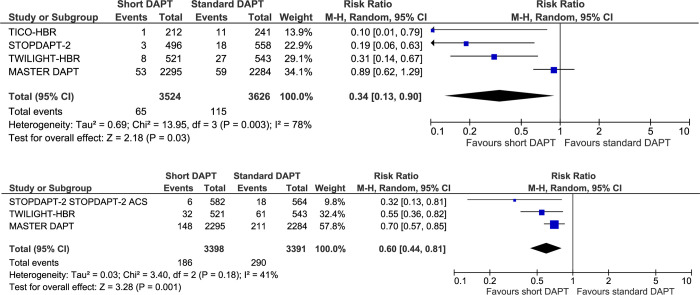
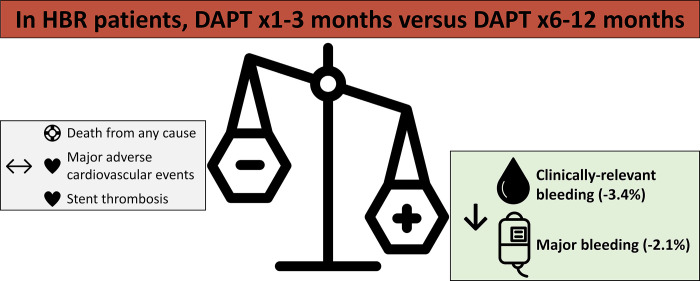
Results: From 503 articles, we included five RCTs (n = 7,242) at overall low risk of bias with median follow-up of 12-months. Compared to standard DAPT, short DAPT did not increase MACE (RR 1.02, 95% CI 0.84-1.23), all-cause death (RR 0.92, 95% CI 0.71-1.20) or stent thrombosis (RR 1.47, 95% CI 0.73-2.93). Short DAPT reduced major bleeding (RR 0.34, 95% CI 0.13-0.90) and the composite of major or clinically-relevant non-major bleeding (RR 0.60, 95% CI 0.44-0.81), translating to 21 and 34 fewer events, respectively, per 1000 patients.
Conclusions: In HBR PCI, DAPT for 1-3 months compared to 6-12 months reduced clinically-relevant bleeding events without jeopardizing ischemic risk. Short DAPT should be considered in HBR patients receiving PCI.
Copyright: © 2023 Bainey et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Short dual antiplatelet therapy in patients with high bleeding risk undergoing percutaneous coronary intervention: a systematic review and meta-analysis.Coron Artery Dis. 2022 Nov 1;33(7):580-589. doi: 10.1097/MCA.0000000000001180. Epub 2022 Sep 22. Coron Artery Dis. 2022. PMID: 36178984
-
Dual antiplatelet therapy duration after percutaneous coronary intervention in high bleeding risk: a meta-analysis of randomized trials.Eur Heart J. 2023 Mar 14;44(11):954-968. doi: 10.1093/eurheartj/ehac706. Eur Heart J. 2023. PMID: 36477292
-
Safety and efficacy of short-term (1 to 3 months) dual antiplatelet therapy in patients undergoing percutaneous coronary interventions: a meta-analysis of randomized controlled trials.J Thromb Thrombolysis. 2020 Nov;50(4):867-873. doi: 10.1007/s11239-020-02069-9. J Thromb Thrombolysis. 2020. PMID: 32607653
-
Dual antiplatelet therapy after percutaneous coronary intervention in patients at high bleeding risk: A systematic review and meta-analysis.Cardiol J. 2023;30(4):556-566. doi: 10.5603/CJ.a2022.0071. Epub 2022 Aug 1. Cardiol J. 2023. PMID: 35912712 Free PMC article.
-
Effectiveness and Safety of Ticagrelor Monotherapy After Short-Duration Dual Antiplatelet Therapy in PCI Patients: A Systematic Review and Meta-Analysis.Am J Cardiol. 2025 Apr 15;241:69-74. doi: 10.1016/j.amjcard.2025.01.014. Epub 2025 Jan 22. Am J Cardiol. 2025. PMID: 39855449
Cited by
-
How to undertake procedures while on antiplatelet agents: a hematologist's view.Res Pract Thromb Haemost. 2024 Aug 5;8(6):102539. doi: 10.1016/j.rpth.2024.102539. eCollection 2024 Aug. Res Pract Thromb Haemost. 2024. PMID: 39318772 Free PMC article. Review.
-
Ultrashort Versus 1-Year Dual Antiplatelet Therapy Following Percutaneous Coronary Intervention: Meta-analysis of Randomized Controlled Trials.J Soc Cardiovasc Angiogr Interv. 2025 Feb 18;4(2):102496. doi: 10.1016/j.jscai.2024.102496. eCollection 2025 Feb. J Soc Cardiovasc Angiogr Interv. 2025. PMID: 40109710 Free PMC article. Review.
-
Abbreviated dual antiplatelet therapy in patients undergoing percutaneous coronary intervention: a systematic review and meta-analysis of randomized controlled trials.BMC Cardiovasc Disord. 2025 Apr 30;25(1):343. doi: 10.1186/s12872-025-04765-x. BMC Cardiovasc Disord. 2025. PMID: 40307711 Free PMC article.
References
-
- Mehta SR, Bainey KR, Cantor WJ, Lordkipanidzé M, Marquis-Gravel G, Robinson SD, et al.. 2018 Canadian Cardiovascular Society/Canadian Association of Interventional Cardiology Focused Update of the Guidelines for the Use of Antiplatelet Therapy. Canadian Journal of Cardiology. 2018;34. doi: 10.1016/j.cjca.2017.12.012 - DOI - PubMed
-
- Costa F, van Klaveren D, James S, Heg D, Räber L, Feres F, et al.. Derivation and validation of the predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score: a pooled analysis of individual-patient datasets from clinical trials. The Lancet. 2017;389: 1025–1034. doi: 10.1016/S0140-6736(17)30397-5 - DOI - PubMed
-
- Hahn JY, Song Y Bin, Oh JH, Chun WJ, Park YH, Jang WJ, et al.. Effect of P2Y12 Inhibitor Monotherapy vs Dual Antiplatelet Therapy on Cardiovascular Events in Patients Undergoing Percutaneous Coronary Intervention: The SMART-CHOICE Randomized Clinical Trial. JAMA. 2019;321: 2428–2437. doi: 10.1001/jama.2019.8146 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
