

Minimum effective concentration of ropivacaine for ultrasound-guided transmuscular quadratus lumborum block in total hip arthroplasty: a randomized clinical trial
- PMID: 37657517
- PMCID: PMC10963918
- DOI: 10.1016/j.bjane.2023.08.005
Minimum effective concentration of ropivacaine for ultrasound-guided transmuscular quadratus lumborum block in total hip arthroplasty: a randomized clinical trial
Abstract
Objective: This trial aimed to identify the Minimum Effective Concentration (MEC90, defined as the concentration which can provide successful block in 90% of patients) of 30 mL ropivacaine for single-shot ultrasound-guided transmuscular Quadratus Lumborum Block (QLB) in patients undergoing Total Hip Arthroplasty (THA).
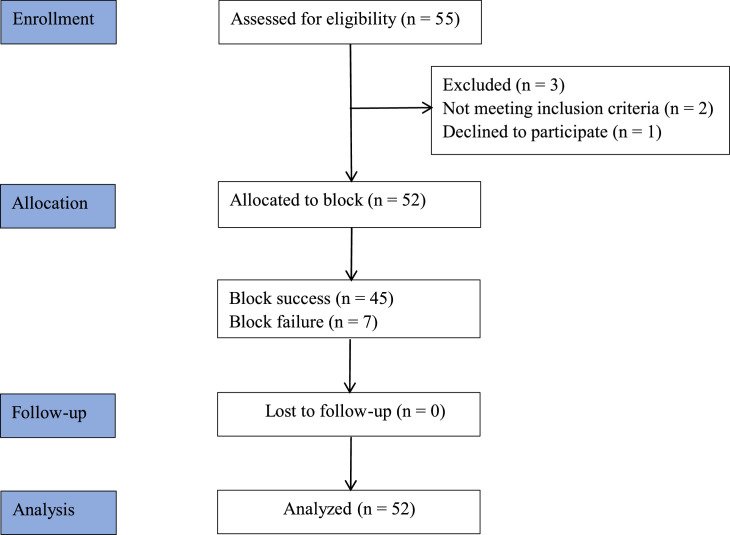
Methods: A double-blind, randomized dose-finding study using the biased coin design up-and-down sequential method, where the concentration of local anesthetic administered to each patient depended on the response from the previous one. Block success was defined as a Numeric Rating Scale (NRS) score during motion ≤ 3 at 6 hours after arrival in the ward. If the block was successful, the next subject received either a 0.025% smaller dose (probability of 0.11) or the same dose (probability of 0.89); otherwise, the next subject received a 0.025% higher ropivacaine concentration. MEC90, MEC95 and MEC99 were estimated by isotonic regression, and the corresponding 95% Confidence Intervals (95% CIs) were calculated by the bootstrapping method.
Results: Based on the analysis of 52 patients, MEC90, MEC95, and MEC99 of ropivacaine for QLB were estimated to be 0.352% (95% CI 0.334-0.372%), 0.363% (95% CI 0.351-0.383%), and 0.373% (95% CI 0.363-0.386%). The concentration of ropivacaine at 0.352% in a volume of 30 ml can provide a successful block in 90% of patients.
Conclusions: For ultrasound-guided transmuscular QLB in patients undergoing THA, 0.352% ropivacaine in a volume of 30 ml can provide a successful block in 90% of patients. Further dose-finding studies and large sample size are required to verify the concentration.
Keywords: Analgesia; Drug dose-response relationship; Nerve block; Ropivacaine; Total hip arthroplasty.
Copyright © 2023. Published by Elsevier España S.L.U.
Conflict of interest statement
Conflicts of interest The authors declare no conflicts of interest.
Figures


 ) and failed (
) and failed ( ) blocks at different ropivacaine concentrations. The horizontal line represents the calculated minimum effective concentration of ropivacaine providing successful transmuscular QLB in 90% of patients (MEC90). Error bars represent the 95% Confidence Interval.
) blocks at different ropivacaine concentrations. The horizontal line represents the calculated minimum effective concentration of ropivacaine providing successful transmuscular QLB in 90% of patients (MEC90). Error bars represent the 95% Confidence Interval.References
-
- Wylde V, Rooker J, Halliday L, et al. Acute postoperative pain at rest after hip and knee arthroplasty: severity, sensory qualities and impact on sleep. Orthop Traumatol Surg Res. 2011;97:139–144. - PubMed
-
- Wylde V, Hewlett S, Learmonth ID, et al. Persistent pain after joint replacement: prevalence, sensory qualities, and postoperative determinants. Pain. 2011;152:566–572. - PubMed
-
- Benyamin R, Trescot AM, Datta S, et al. Opioid complications and side effects. Pain Physician. 2008;11(2 Suppl):S105–S120. - PubMed
-
- Harirforoosh S, Asghar W, Jamali F. Adverse effects of nonsteroidal antiinflammatory drugs: an update of gastrointestinal, cardiovascular and renal complications. J Pharm Pharm Sci. 2013;16:821–847. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
