

Diffusion tensor imaging of the physis: the ABC's
- PMID: 37658251
- PMCID: PMC10859915
- DOI: 10.1007/s00247-023-05753-z
Diffusion tensor imaging of the physis: the ABC's
Abstract
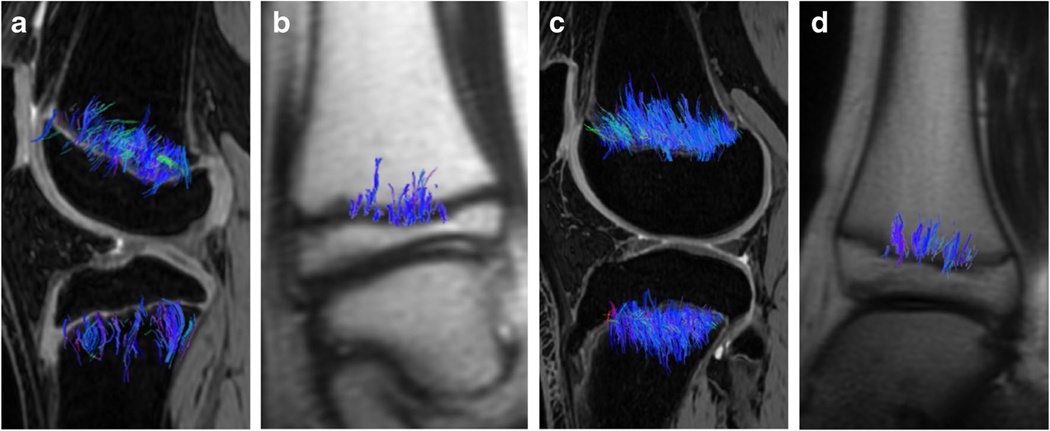
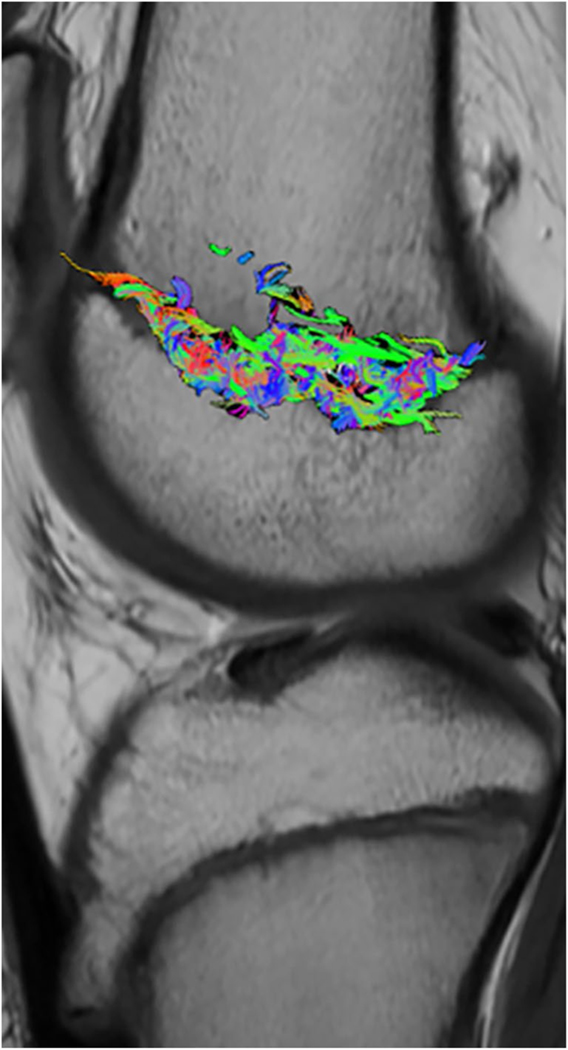
The physis, or growth plate, is the primary structure responsible for longitudinal growth of the long bones. Diffusion tensor imaging (DTI) is a technique that depicts the anisotropic motion of water molecules, or diffusion. When diffusion is limited by cellular membranes, information on tissue microstructure can be acquired. Tractography, the visual display of the direction and magnitude of water diffusion, provides qualitative visualization of complex cellular architecture as well as quantitative diffusion metrics that appear to indirectly reflect physeal activity. In the growing bones, DTI depicts the columns of cartilage and new bone in the physeal-metaphyseal complex. In this "How I do It", we will highlight the value of DTI as a clinical tool by presenting DTI tractography of the physeal-metaphyseal complex of children and adolescents during normal growth, illustrating variation in qualitative and quantitative tractography metrics with age and skeletal location. In addition, we will present tractography from patients with physeal dysfunction caused by growth hormone deficiency and physeal injury due to trauma, chemotherapy, and radiation therapy. Furthermore, we will delineate our process, or "DTI pipeline," from image acquisition to data interpretation.
Keywords: Anisotropy; Child; Diffusion tensor imaging; Growth plate; Magnetic resonance imaging; Physis; Tractography.
© 2023. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
Figures
















Comment in
-
Commentary: MR-DTI of the growth plate: redefining concepts and evaluating future perspectives.Pediatr Radiol. 2025 Feb;55(2):360-362. doi: 10.1007/s00247-024-06123-z. Epub 2024 Dec 21. Pediatr Radiol. 2025. PMID: 39708152 No abstract available.
References
-
- Kvist O (2022) Magnetic resonance imaging and advanced imaging assessment of the growth plate in the adolescent and young adult. Karolinska Institute Press, Stockholm
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
