

Validating the measurement of upper limb sensorimotor behavior utilizing a tablet in neurologically intact controls and individuals with chronic stroke
- PMID: 37658432
- PMCID: PMC10474703
- DOI: 10.1186/s12984-023-01240-6
Validating the measurement of upper limb sensorimotor behavior utilizing a tablet in neurologically intact controls and individuals with chronic stroke
Abstract
Background: Intact sensorimotor function of the upper extremity is essential for successfully performing activities of daily living. After a stroke, upper limb function is often compromised and requires rehabilitation. To develop appropriate rehabilitation interventions, sensitive and objective assessments are required. Current clinical measures often lack precision and technological devices (e.g. robotics) that are objective and sensitive to small changes in sensorimotor function are often unsuitable and impractical for performing home-based assessments. Here we developed a portable, tablet-based application capable of quantifying upper limb sensorimotor function after stroke. Our goal was to validate the developed application and accompanying data analysis against previously validated robotic measures of upper limb function in stroke.
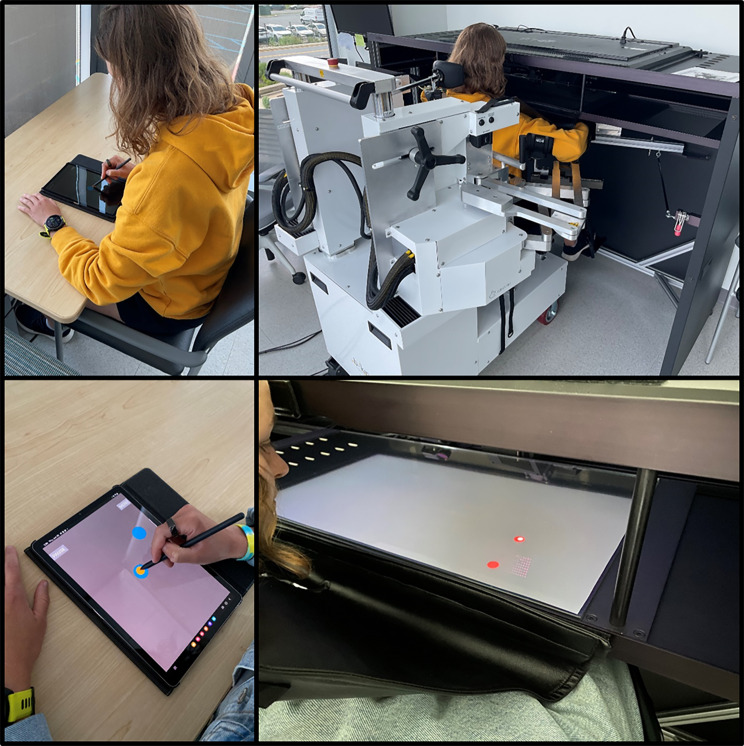
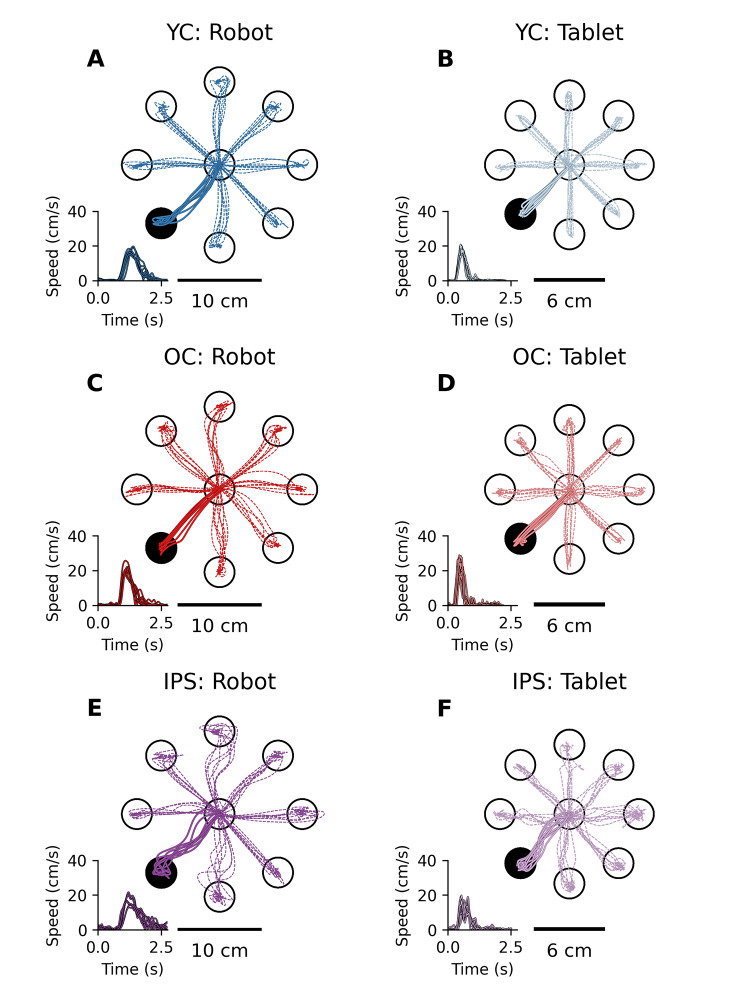
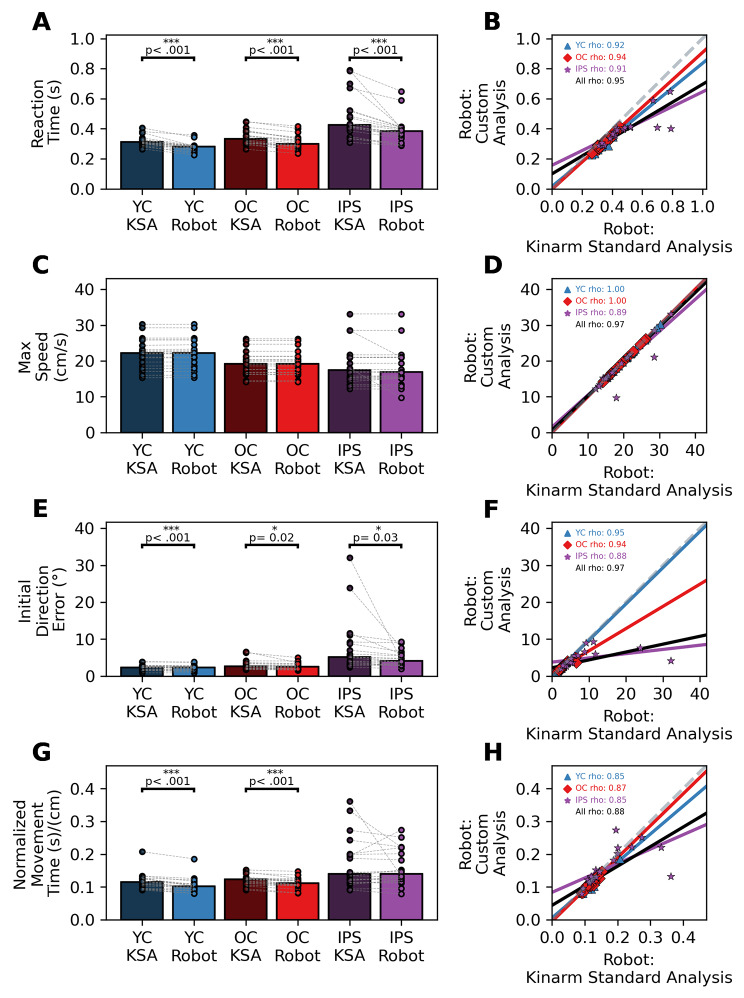
Methods: Twenty individuals with stroke, twenty age-matched older controls, and twenty younger controls completed an eight-target Visually Guided Reaching (VGR) task using a Kinarm Robotic Exoskeleton and a Samsung Galaxy Tablet. Participants completed eighty trials of the VGR task on each device, where each trial consisted of making a reaching movement to one of eight pseudorandomly appearing targets. We calculated several outcome parameters capturing various aspects of sensorimotor behavior (e.g., Reaction Time, Initial Direction Error, Max Speed, and Movement Time) from each reaching movement, and our analyses compared metric consistency between devices. We used the previously validated Kinarm Standard Analysis (KSA) and a custom in-house analysis to calculate each outcome parameter.
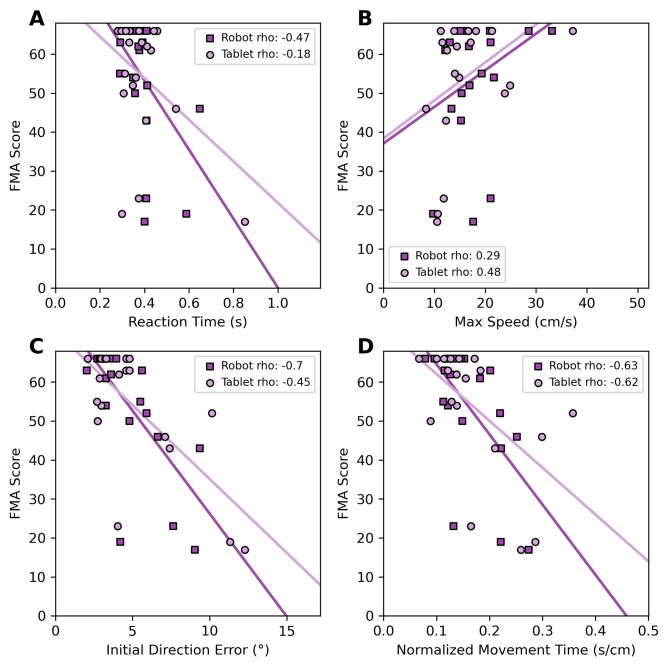
Results: We observed strong correlations between the KSA and our custom analysis for all outcome parameters within each participant group, indicating our custom analysis accurately replicates the KSA. Minimal differences were observed for between-device comparisons (tablet vs. robot) in our outcome parameters. Additionally, we observed similar correlations for each device when comparing the Fugl-Meyer Assessment (FMA) scores of individuals with stroke to tablet-derived metrics, demonstrating that the tablet can capture clinically-based elements of upper limb impairment.
Conclusions: Tablet devices can accurately assess upper limb sensorimotor function in neurologically intact individuals and individuals with stroke. Our findings validate the use of tablets as a cost-effective and efficient assessment tool for upper-limb function after stroke.
Keywords: Assessment; Reaching; Robotics; Sensorimotor; Stroke; Tablet.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, Boehme AK, Buxton AE, Carson AP, Commodore-Mensah Y, Elkind MSV, Evenson KR, Eze-Nliam C, Ferguson JF, Generoso G, Ho JE, Kalani R, Khan SS, Kissela BM, Knutson KL, Levine DA, Lewis TT, Liu J, Loop MS, Ma J, Mussolino ME, Navaneethan SD, Perak AM, Poudel R, Rezk-Hanna M, Roth GA, Schroeder EB, Shah SH, Thacker EL, VanWagner LB, Virani SS, Voecks JH, Wang NY, Yaffe K, Martin SS, on behalf of the American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation [Internet]. 2022 Feb 22 [cited 2022 Jul 26];145(8). 10.1161/CIR.0000000000001052. - PubMed
-
- Rathore SS, Hinn AR, Cooper LS, Tyroler HA, Rosamond WD. Characterization of incident stroke signs and symptoms: findings from the atherosclerosis risk in Communities Study. Stroke. 2002;33(11):2718–21. - PubMed
-
- Kwakkel G, Kollen BJ, van der Grond J, Prevo AJH. Probability of regaining dexterity in the Flaccid Upper Limb: impact of severity of Paresis and Time since Onset in Acute Stroke. Stroke. 2003;34(9):2181–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
