

Treatment of pelvic giant cell tumor by wide resection with patient-specific bone-cutting guide and reconstruction with 3D-printed personalized implant
- PMID: 37658436
- PMCID: PMC10472683
- DOI: 10.1186/s13018-023-04142-4
Treatment of pelvic giant cell tumor by wide resection with patient-specific bone-cutting guide and reconstruction with 3D-printed personalized implant
Abstract
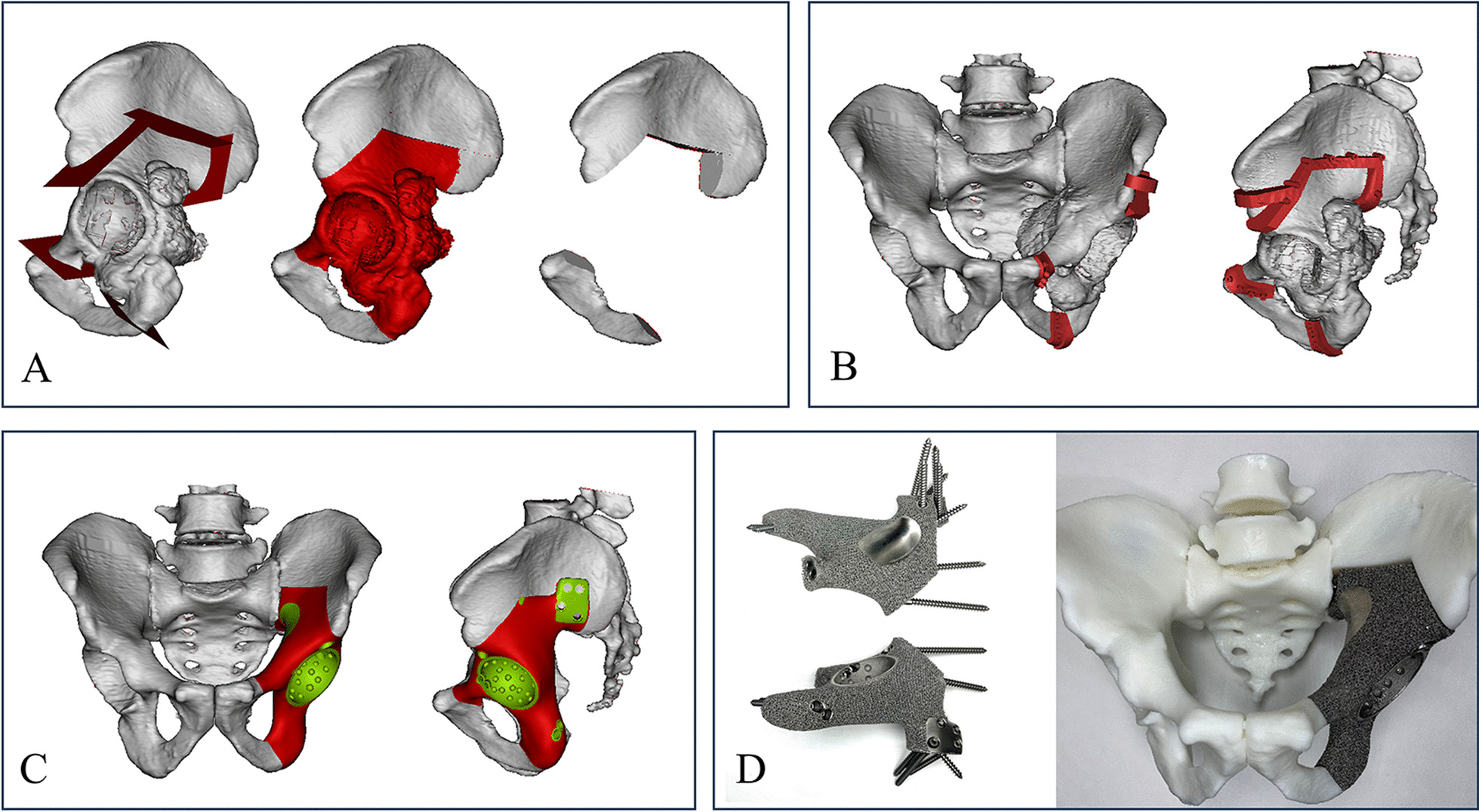
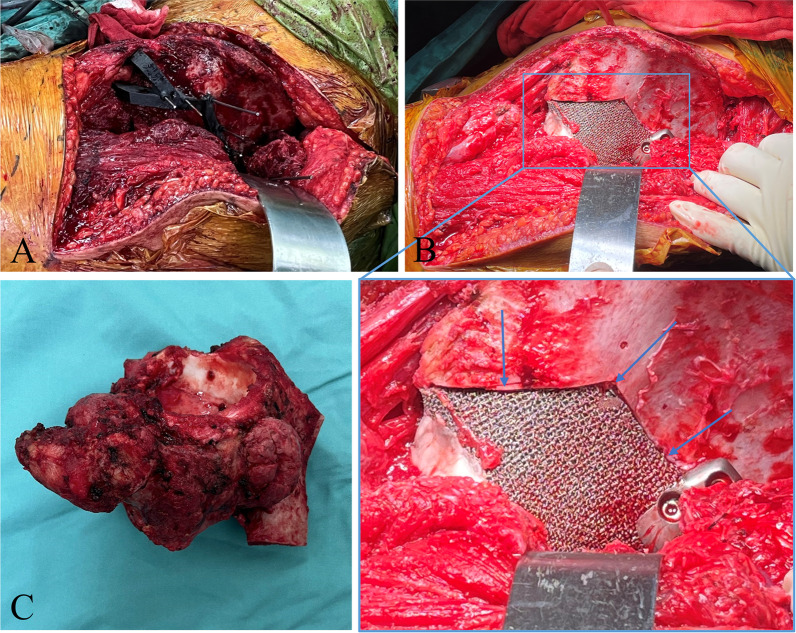
Background: This study reports our experience in the treatment of aggressive pelvic GCT through wide resection assisted with patient-specific bone-cutting guides (PSBCGs) and subsequent reconstruction with 3D-printed personalized implants (3DPIs), aiming to present the operative technique of this method and evaluate its clinical efficacy.
Methods: We retrospectively analyzed seven patients who underwent wide resection of pelvic GCT followed by reconstruction with 3DPIs from August 2019 to February 2021. There were two males and five females, with a mean age of 43 years. PSBCGs and 3DPIs were prepared using 3D-printing technology. The operational outcomes, local recurrence, radiological results, and any associated complications of this technique were assessed. And the functional outcomes were assessed according to the Musculoskeletal Tumor Society (MSTS) 93 functional score.
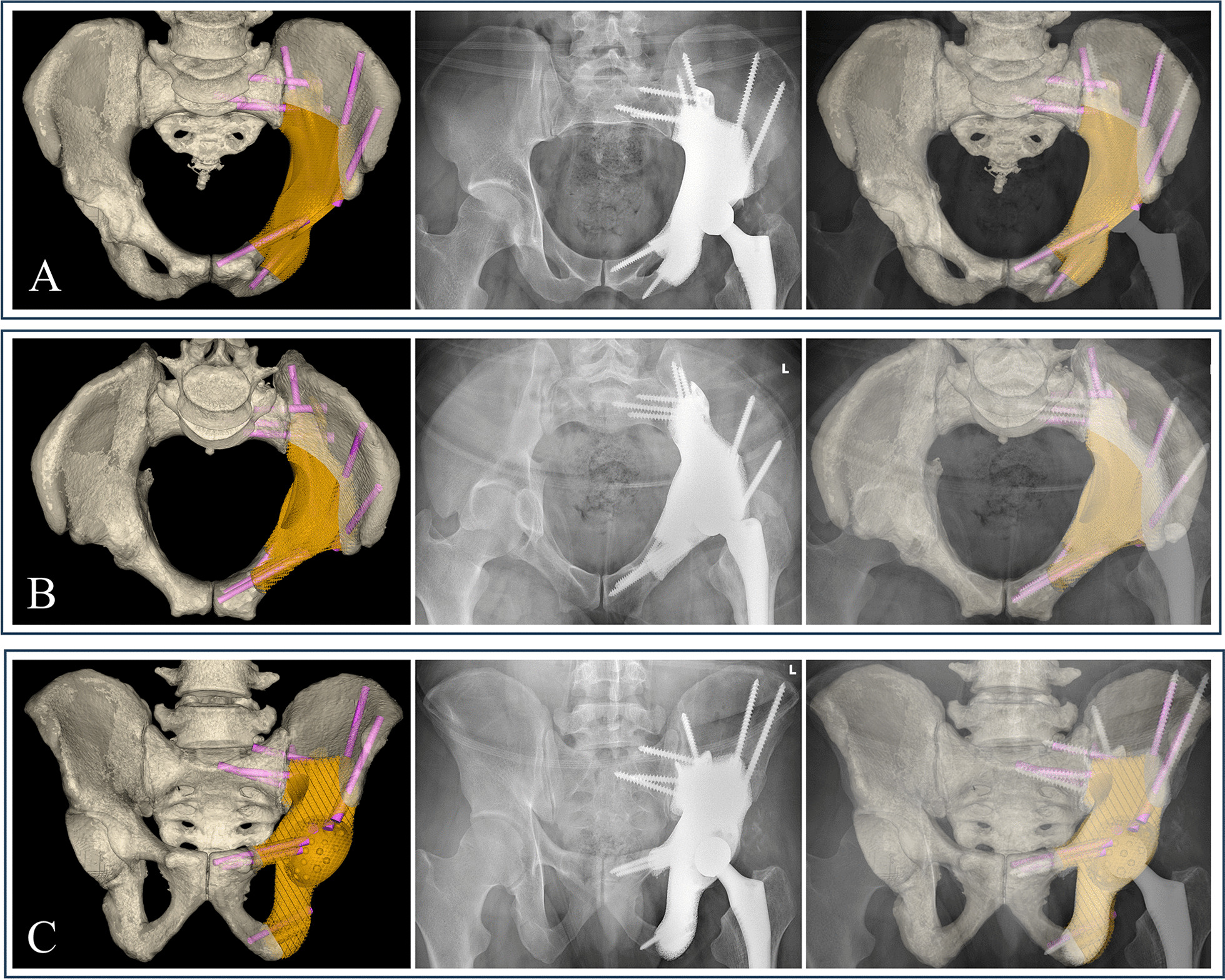
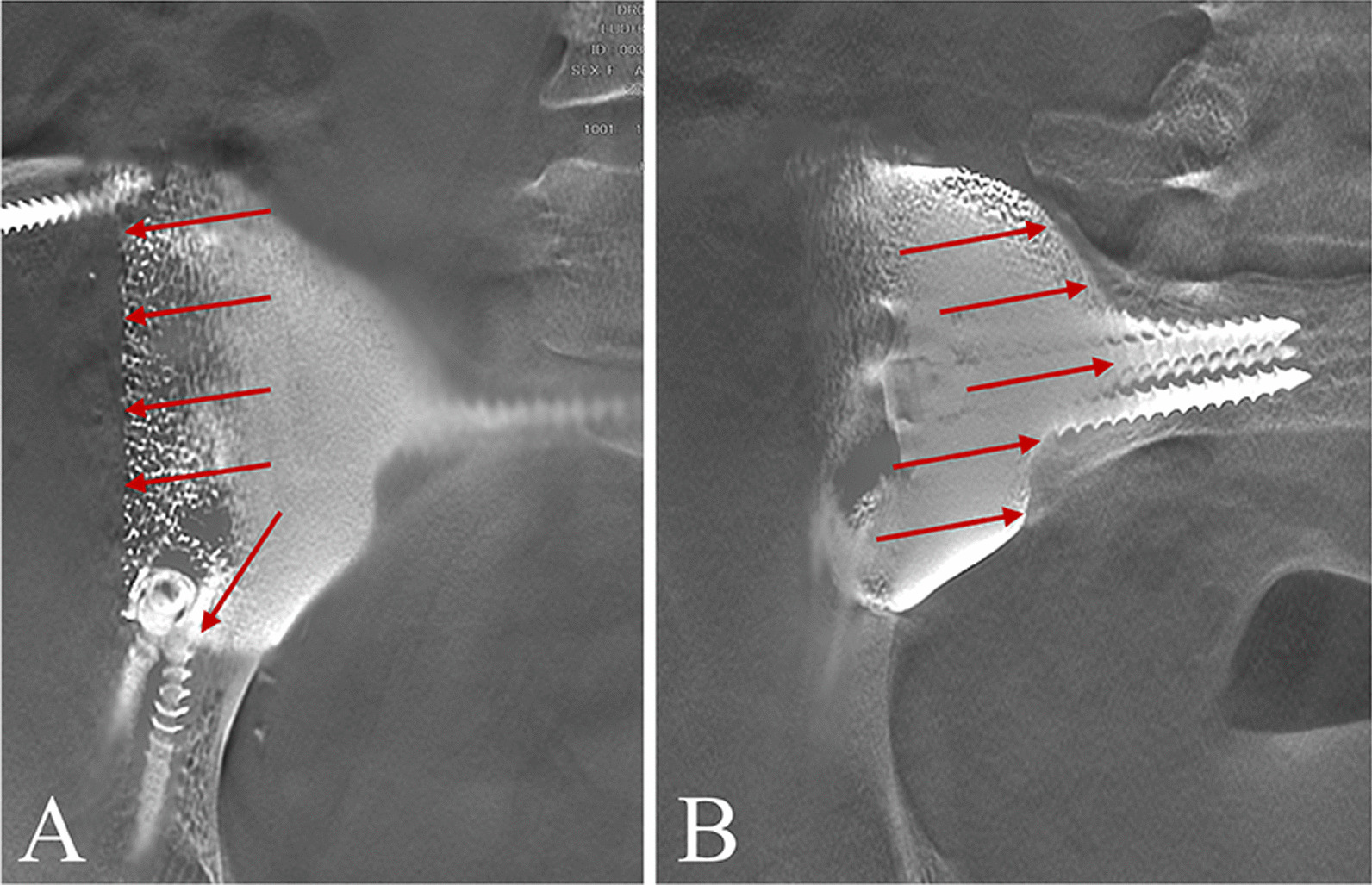
Results: The mean follow-up time was 35.3 months (range 28-45 months). There was no intraoperative complication. Negative surgical margins were achieved in all patients. Postoperative pelvic radiographs showed that 3DPIs matched the shape and size of the bone defect. The anterior-posterior, inlet, and outlet pelvic radiograph demonstrated precise reconstruction consistent with the surgical planning. In addition, tomosynthesis-Shimadzu metal artifact reduction technology (T-SMART) showed good osseointegration at an average of three months after surgery (range 2-4 months). There was no local recurrence or tumor metastasis. The average MSTS score was 24.4 (range 23-27) at the last follow-up. Delayed wound healing was observed in one patient, and the wounds healed after debridement. Prosthesis-related complications were not detected during the follow-up, such as aseptic loosening or structure failure.
Conclusions: The treatment of aggressive pelvic GCTs through wide resection assisted with PSBCGs and subsequent reconstruction with 3DPIs is a feasible method, which provides good clinical results and reasonable functional outcomes.
Keywords: 3D-printed implant; Osseointegration; Patient-specific bone-cutting guide; Pelvic GCT.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Picci P, Manfrini M, Fabbri N, Gambarotti M, Vanel D: Atlas of musculoskeletal tumors and tumorlike lesions: the Rizzoli case archive: Springer Science & Business Media; 2014.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
