

Studying temporal titre evolution of commercial SARS-CoV-2 assays reveals significant shortcomings of using BAU standardization for comparison
- PMID: 37658454
- PMCID: PMC10474769
- DOI: 10.1186/s12985-023-02167-z
Studying temporal titre evolution of commercial SARS-CoV-2 assays reveals significant shortcomings of using BAU standardization for comparison
Abstract
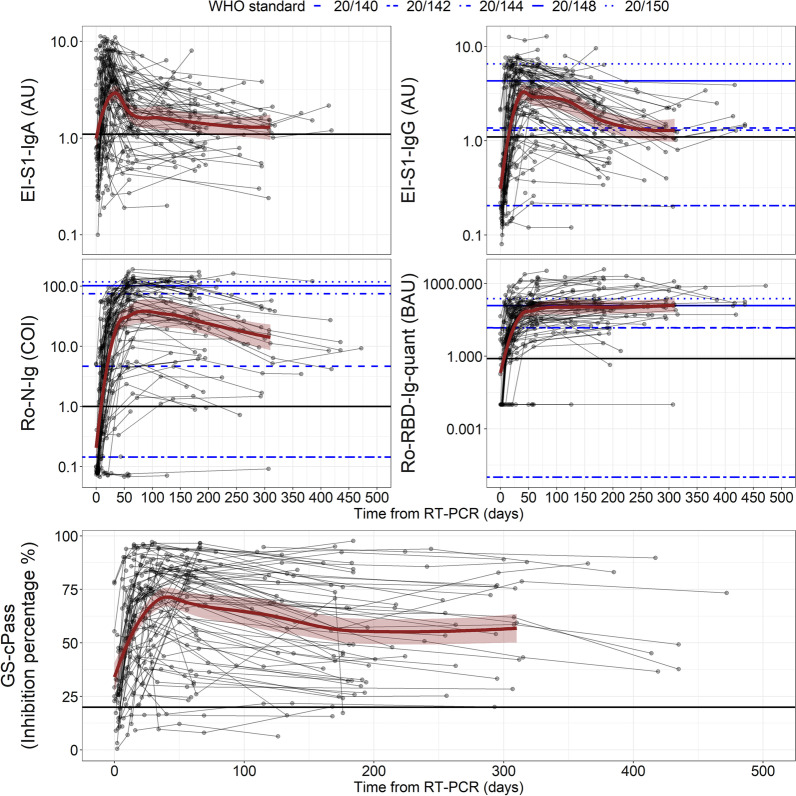
Background: Measuring specific anti-SARS-CoV-2 antibodies has become one of the main epidemiological tools to survey the ongoing SARS-CoV-2 pandemic, but also vaccination response. The WHO made available a set of well-characterized samples derived from recovered individuals to allow normalization between different quantitative anti-Spike assays to defined Binding Antibody Units (BAU).
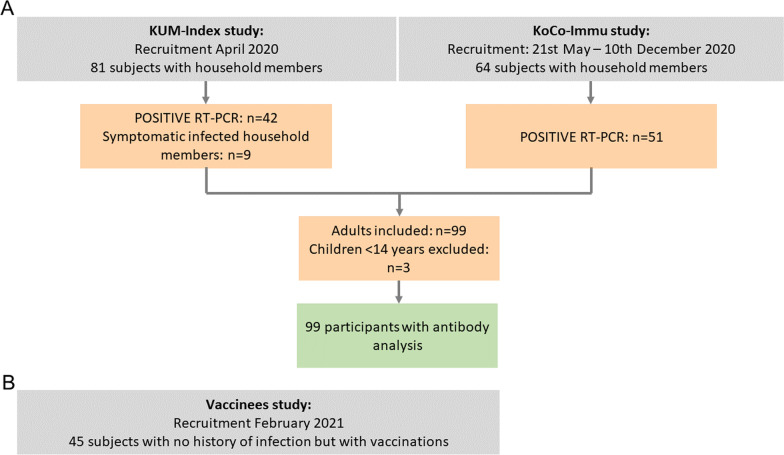
Methods: To assess sero-responses longitudinally, a cohort of ninety-nine SARS-CoV-2 RT-PCR positive subjects was followed up together with forty-five vaccinees without previous infection but with two vaccinations. Sero-responses were evaluated using a total of six different assays: four measuring anti-Spike proteins (converted to BAU), one measuring anti-Nucleocapsid proteins and one SARS-CoV-2 surrogate virus neutralization. Both cohorts were evaluated using the Euroimmun Anti-SARS-CoV-2-ELISA anti-S1 IgG and the Roche Elecsys Anti-SARS-CoV-2 anti-S1 assay.
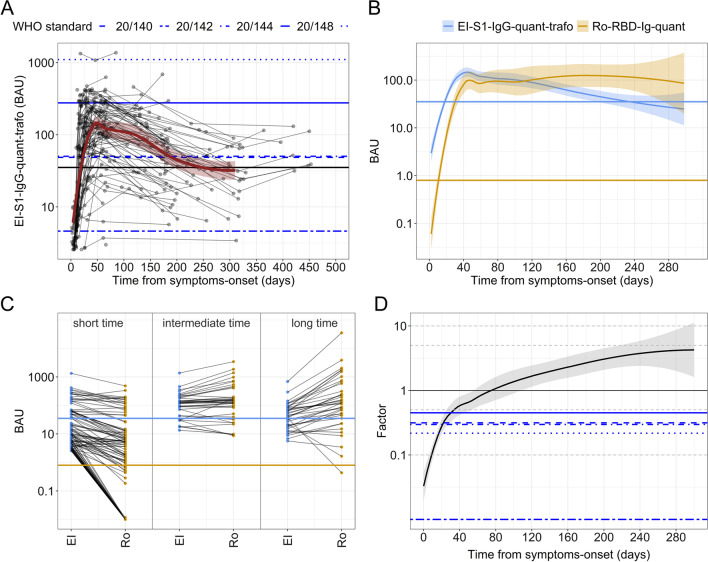
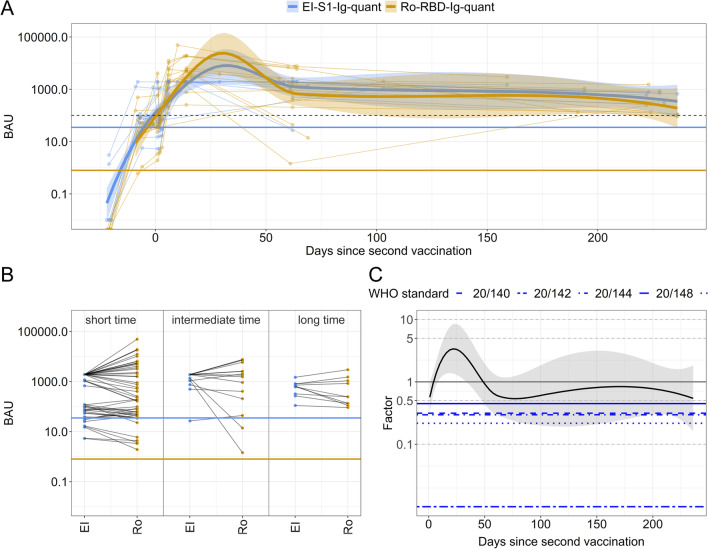
Results: In SARS-CoV-2-convalesce subjects, the BAU-sero-responses of Euroimmun Anti-SARS-CoV-2-ELISA anti-S1 IgG and Roche Elecsys Anti-SARS-CoV-2 anti-S1 peaked both at 47 (43-51) days, the first assay followed by a slow decay thereafter (> 208 days), while the second assay not presenting any decay within one year. Both assay values in BAUs are only equivalent a few months after infection, elsewhere correction factors up to 10 are necessary. In contrast, in infection-naive vaccinees the assays perform similarly.
Conclusion: The results of our study suggest that the establishment of a protective correlate or vaccination booster recommendation based on different assays, although BAU-standardised, is still challenging. At the moment the characteristics of the available assays used are not related, and the BAU-standardisation is unable to correct for that.
Keywords: Antibody; Binding antibody units; COVID-19; Nucleocapsid; RBD; SARS-CoV-2; Serology; Spike.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
AW and MH report personal fees and non-financial support from Roche Diagnostics, LO reports non-financial support from Roche Diagnostics. AW, MH and LO report non-financial support from Euroimmun, non-financial support from Viramed, non-financial support from Mikrogen. AW, MH, LO report grants, non-financial support and other from German Centre for Infection Research DZIF, grants and non-financial support from Government of Bavaria, non-financial support from BMW, non-financial support from Munich Police, nonfinancial support and other from Accenture. MH and AW report personal fees and nonfinancial support from Dr. Box-Betrobox, non-financial support from Dr. Becker MVZ during the conduct of the study. AW is involved in other different patents and companies not in relation with the serology of SARS-CoV-2. AW reports personal fees and other from Haeraeus Sensors, nonfinancial support from Bruker Daltonics, all of which are outside the submitted work, and non-related to SARS-CoV-2.
Figures
References
-
- WHO. Coronavirus disease (COVID-19) pandemic. 01 July 2022. https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
-
- CSSE. Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU) COVID-19 dashboard. 01 July 2022 https://coronavirus.jhu.edu/map.html.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
