

Metformin Overcomes the Consequences of NKX3.1 Loss to Suppress Prostate Cancer Progression
- PMID: 37659962
- PMCID: PMC10902192
- DOI: 10.1016/j.eururo.2023.07.016
Metformin Overcomes the Consequences of NKX3.1 Loss to Suppress Prostate Cancer Progression
Abstract
Background: The antidiabetic drug metformin has known anticancer effects related to its antioxidant activity; however, its clinical benefit for prostate cancer (PCa) has thus far been inconclusive. Here, we investigate whether the efficacy of metformin in PCa is related to the expression status of NKX3.1, a prostate-specific homeobox gene that functions in mitochondria to protect the prostate from aberrant oxidative stress.
Objective: To investigate the relationship of NKX3.1 expression and metformin efficacy in PCa.
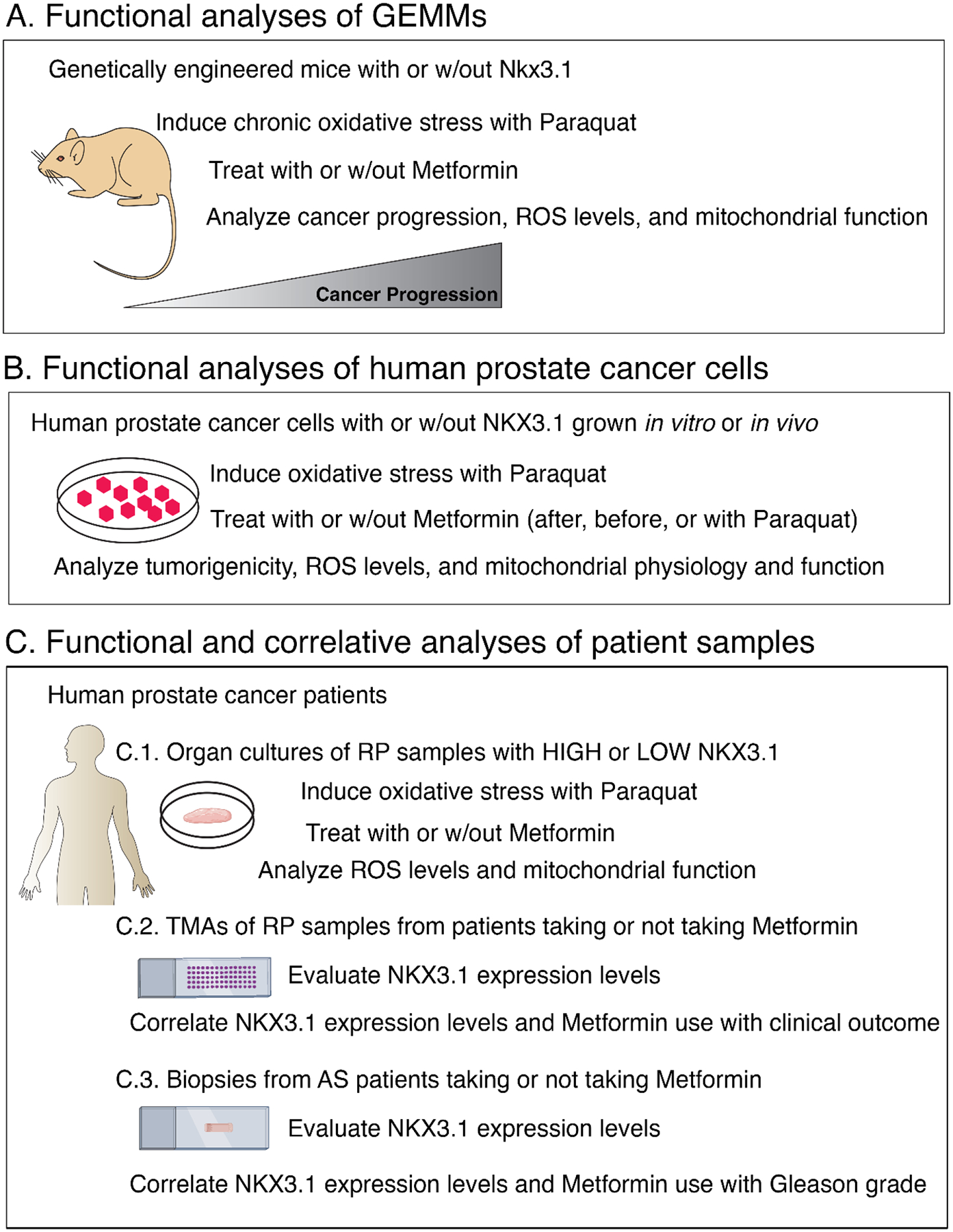
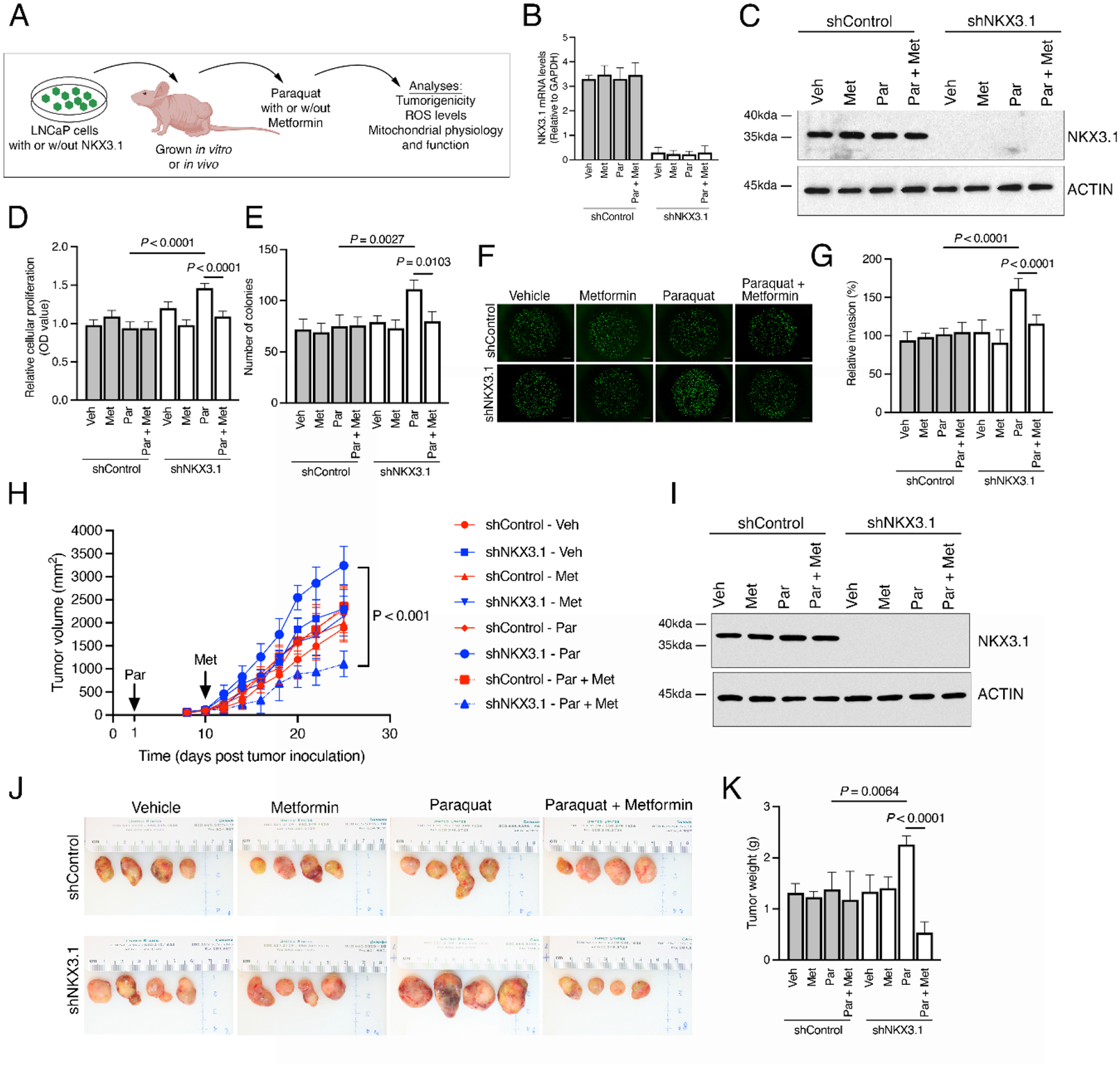
Design, setting, and participants: Functional studies were performed in vivo and in vitro in genetically engineered mouse models and human LNCaP cells, and organotypic cultures having normal or reduced/absent levels of NKX3.1. Correlative studies were performed using two independent retrospective tissue microarray cohorts of radical prostatectomies and a retrospective cohort of prostate biopsies from patients on active surveillance.
Intervention: Metformin was administered before or after the induction of oxidative stress by treatment with paraquat.
Outcome measurements and statistical analysis: Functional endpoints included analyses of histopathology, tumorigenicity, and mitochondrial function. Correlative endpoints include Kaplan-Meier curves and Cox proportional hazard regression models.
Results and limitations: Metformin reversed the adverse consequences of NKX3.1 deficiency following oxidative stress in vivo and in vitro, as evident by reduced tumorigenicity and restored mitochondrial function. Patients with low NKX3.1 expression showed a significant clinical benefit from taking metformin.
Conclusions: Metformin can overcome the adverse consequences of NKX3.1 loss for PCa progression by protecting against oxidative stress and promoting normal mitochondrial function. These functional activities and clinical correlates were observed only with low NKX3.1 expression. Thus, the clinical benefit of metformin in PCa may depend on the status of NKX3.1 expression.
Patient summary: Prostate cancer patients with low NKX3.1 are likely to benefit most from metformin treatment to delay disease progression in a precision interception paradigm.
Keywords: Metformin; Mitochondria; NKX3.1; Oxidative stress; Precision medicine; Prostate cancer.
Copyright © 2023 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures



Comment in
-
About metformin and its action on the mitochondrial respiratory chain in prostate cancer.Transl Androl Urol. 2024 May 31;13(5):909-914. doi: 10.21037/tau-23-602. Epub 2024 May 16. Transl Androl Urol. 2024. PMID: 38855601 Free PMC article. No abstract available.
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin 2022;72:7–33. - PubMed
-
- Lovf M, Zhao S, Axcrona U, et al. Multifocal primary prostate cancer exhibits high degree of genomic heterogeneity. Eur Urol 2019;75:498–505. - PubMed
-
- Sartor O, de Bono JS. Metastatic prostate cancer. N Engl J Med 2018;378:645–57. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
