

ONCOS-102 plus pemetrexed and platinum chemotherapy in malignant pleural mesothelioma: a randomized phase 2 study investigating clinical outcomes and the tumor microenvironment
- PMID: 37661097
- PMCID: PMC10476122
- DOI: 10.1136/jitc-2023-007552
ONCOS-102 plus pemetrexed and platinum chemotherapy in malignant pleural mesothelioma: a randomized phase 2 study investigating clinical outcomes and the tumor microenvironment
Abstract
Background: ONCOS-102, an oncolytic adenovirus expressing granulocyte-macrophage colony-stimulating factor, can alter the tumor microenvironment to an immunostimulatory state. Combining ONCOS-102 with standard-of-care chemotherapy for malignant pleural mesothelioma (MPM) may improve treatment outcomes.
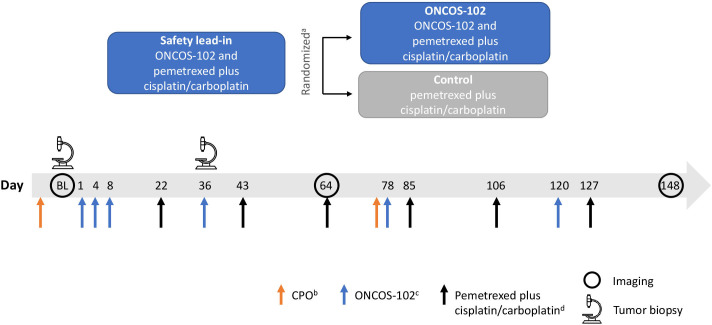
Methods: In this open-label, randomized study, patients with unresectable MPM received intratumoral ONCOS-102 (3×1011 virus particles on days 1, 4, 8, 36, 78, and 120) and pemetrexed plus cisplatin/carboplatin (from day 22), or pemetrexed plus cisplatin/carboplatin alone. The primary endpoint was safety. Overall survival (OS), progression-free survival, objective response rate, and tumor immunologic activation (baseline and day 36 biopsies) were also assessed.
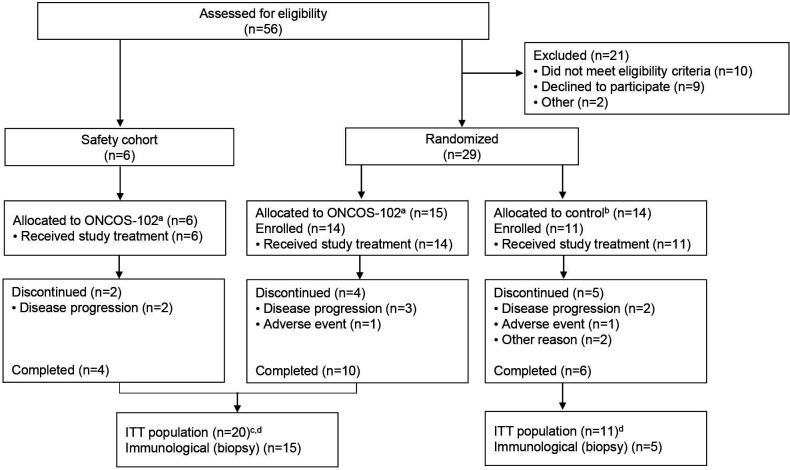
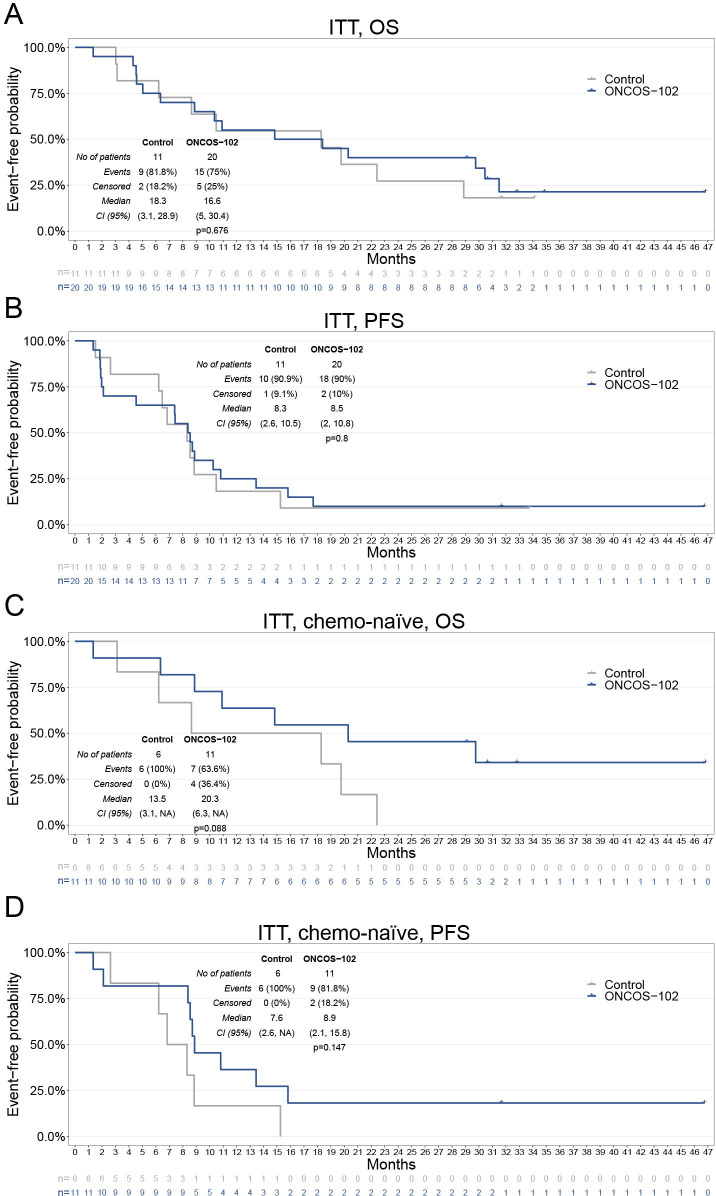
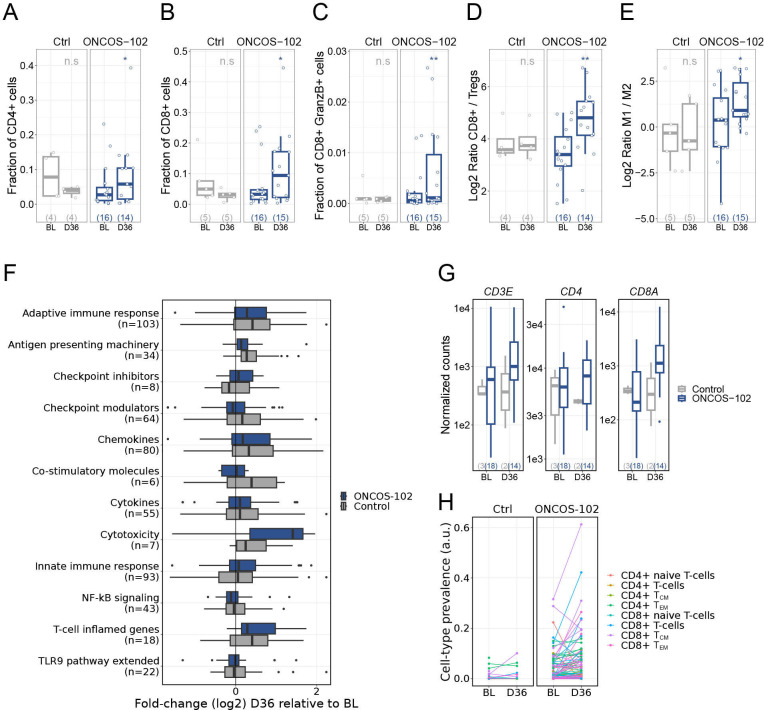
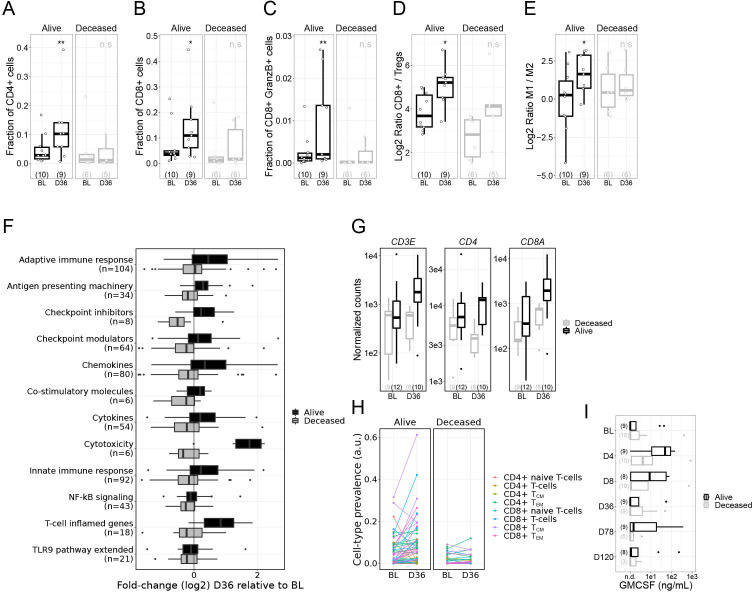
Results: In total, 31 patients (safety lead-in: n=6, randomized: n=25) were enrolled. Anemia (15.0% and 27.3%) and neutropenia (40.0% and 45.5%) were the most frequent grade ≥3 adverse events (AEs) in the ONCOS-102 (n=20) and chemotherapy-alone (n=11) cohorts. No patients discontinued ONCOS-102 due to AEs. No statistically significant difference in efficacy endpoints was observed. There was a numerical improvement in OS (30-month OS rate 34.1% vs 0; median OS 20.3 vs 13.5 months) with ONCOS-102 versus chemotherapy alone in chemotherapy-naïve patients (n=17). By day 36, ONCOS-102 was associated with increased T-cell infiltration and immune-related gene expression that was not observed in the control cohort. Substantial immune activation in the tumor microenvironment was associated with survival at month 18 in the ONCOS-102 cohort.
Conclusions: ONCOS-102 plus pemetrexed and cisplatin/carboplatin was well tolerated by patients with MPM. In injected tumors, ONCOS-102 promoted a proinflammatory environment, including T-cell infiltration, which showed association with survival at month 18.
Keywords: T-lymphocytes; immunomodulation; oncolytic viruses; therapies, investigational; tumor microenvironment.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: SP reports leadership/fiduciary role for Pegasys, and patent for lurbinectidin plus atezolizumab. CR reports personal payments from Bristol Meyers Squibb, MSD, and Takeda. NI reports honoraria from Amgen, Bristol Meyers Squibb, Daiichi Sankyo, Eisai, Glaxo Smith Klein, and Lilly; support for meeting attendance from Gilead, Novartis, Pfizer, PharmaMar, and Roche Genentech; and Data Safety Monitoring Board/Advisory Board participation for Transgene. SViteri reports fees from Abbvie, AstraZeneca, Bristol Meyers Squibb, Merck, Ipsen, MSD, OSE Immunotherapeutics, Puma Biotech, Roche, and Takeda. MH-J reports honoraria from AstraZeneca and support for meeting attendance from Roche and Takeda. AM-M reports honoraria from AstraZeneca/MedImmune, Bristol Myers Squibb, F. Hoffmann La Roche AG, MSD, MSD oncology, and Pfizer. AN reports consulting fees/honoraria from Amgen, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Pfizer, Roche, Takeda; fees for expert testimony from Medsir and Oryzon; Data Safety Monitoring Board participation for Hengenix, and support for meeting attendance from Boehringer Ingelheim, Pfizer, and Roche. SC, ML and XS report no potential conflicts of interest to disclose. JZ reports research grants from AstraZeneca, Bristol Myers Squibb, and Roche; consulting fees from Bristol Myers Squibb, Novartis and Sanofi, honoraria from AstraZeneca, Bristol Myers Squibb, MSD, NanoString, Roche, and Sanofi; and support for meeting attendance from AstraZeneca, Bristol Myers Squibb, Roche, and Sanofi. SVetrhus and MJ report prior employment by Circio Holding ASA and stock in Circio Holding ASA. TBH reports employment by Circio Holding ASA and stock in Circio Holding ASA. VL reports employment with Servier, consultancy fees from Athebio AG, CatalYm, and Circio Holding ASA; and stock in Circio Holding ASA. LP-A reports grants/contracts from AstraZeneca, Bristol Meyers Squibb, MSD, and Pfizer; consulting fees from Amgen, AstraZeneca, Bayer, Bristol Meyers Squibb, GSK, Janssen, Lilly, Mirati Therapeutics, Novartis, Merck, MSD, Pfizer, Pharmamar, Roche, Daiichi Sankyo, Sanofi, Servier, and Takeda, and honoraria from AstraZeneca, Janssen, Merck, and Mirati Therapeutics.
Figures
References
-
- Davis A, Ke H, Kao S, et al. An update on emerging therapeutic options for malignant pleural mesothelioma. Lung Cancer (Auckl) 2022;13:1–12. 10.2147/LCTT.S288535 Available: https://10.2147/LCTT.S288535 - DOI - PMC - PubMed
-
- Klebe S, Hocking AJ, Soeberg M, et al. The significance of short latency in mesothelioma for attribution of causation: report of a case with predisposing germline mutations and review of the literature. Int J Environ Res Public Health 2021;18:13310. 10.3390/ijerph182413310 Available: https://10.3390/ijerph182413310 - DOI - PMC - PubMed
-
- Kwak K, Cho SI, Paek D. Future incidence of malignant mesothelioma in South Korea: updated projection to 2038. Int J Environ Res Public Health 2021;18:6614. 10.3390/ijerph18126614 Available: https://10.3390/ijerph18126614 - DOI - PMC - PubMed
-
- Metro G, Signorelli D, Pizzutilo EG, et al. Immune checkpoint inhibitors for unresectable malignant pleural mesothelioma. Hum Vaccin Immunother 2021;17:2972–80. 10.1080/21645515.2021.1917933 Available: https://10.1080/21645515.2021.1917933 - DOI - PMC - PubMed
-
- Shavelle R, Vavra-Musser K, Lee J, et al. Life expectancy in pleural and peritoneal mesothelioma. Lung Cancer Int 2017;2017:2782590. 10.1155/2017/2782590 Available: https://10.1155/2017/2782590 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical