

[Side effects of immune checkpoint inhibitor therapy : What intensive care specialists need to know]
- PMID: 37661230
- PMCID: PMC10901948
- DOI: 10.1007/s00063-023-01057-0
[Side effects of immune checkpoint inhibitor therapy : What intensive care specialists need to know]
Abstract
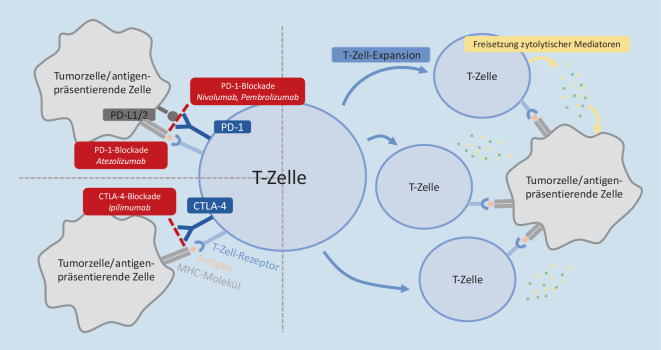
Immunotherapies, and in particular checkpoint inhibitors, have revolutionized the treatment of cancer. However, due to their mechanism of action, the activation of the body's own T cells, side effects are frequently associated with these therapies. So-called immune-related adverse events (irAEs) manifest as autoimmunological phenomena, can occur in any organ system, and even lead to severe organ failure. Due to the time latency of up to months after administration of a checkpoint inhibitor until the first manifestation of an irAE, it is essential to consider a therapy-specific adverse event at any time during therapy. In case of incipient organ failure, discontinuation of the checkpoint inhibitor and rapid initiation of high-dose corticosteroid therapy is essential, which, in the absence of response, should be extended by further immunosuppressive or anti-inflammatory therapies. In general, the response to corticosteroids and extended therapy options is good, and in this sense organ failure is often reversible. Nevertheless, intensive medical care with the possible need for organ-supporting therapies should only be provided strictly according to the patient's wishes and in close consultation with the hematologist/oncologist in charge. Because of the great therapeutic benefit of immunotherapies, their frequent use, and potential to be used in curative lines of therapy in the future, intensive care physicians will also be confronted more frequently with irAEs after checkpoint inhibition. Accordingly, understanding, recognizing, and treating side effects after immunotherapies is increasingly essential for intensivists.
Immuntherapien, und insbesondere Immuncheckpointinhibitoren, haben die Behandlung maligner Erkrankungen revolutioniert. Ihrem Wirkmechanismus geschuldet, der Aktivierung körpereigener T‑Zellen, sind jedoch auch häufig Nebenwirkungen die Folge einer Therapie. Sogenannte immunmediierte Nebenwirkungen („immune-related adverse event“, irAE) manifestieren sich als autoimmunologische Phänomene, können in jedem Organsystem auftreten und bis hin zu schwerem Organversagen führen. Aufgrund der zeitlichen Latenz von bis zu Monaten nach Verabreichung eines Checkpointinhibitors bis zur Erstmanifestation einer irAE ist es essenziell, bei entsprechender stattgehabter Therapie zu jedem Zeitpunkt an eine therapiespezifische Nebenwirkung zu denken. Bei beginnendem Organversagen ist das Absetzen des Checkpointinhibitors sowie der rasche Beginn mit einer Hochdosiskortisontherapie essenziell, die bei fehlendem Ansprechen um weitere Immunsuppressiva oder antiinflammatorische Therapieoptionen erweitert werden soll. Generell ist das Ansprechen auf Kortikosteroide und erweiterte Therapieoptionen gut und in diesem Sinne das Organversagen auch oft reversibel. Eine intensivmedizinische Betreuung mit etwaiger Notwendigkeit organunterstützender Therapien sollte dennoch nur streng nach Patient:innenwunsch sowie in enger Rücksprache mit den betreuenden Hämatoonkolog:innen erfolgen. Mit dem großen therapeutischen Nutzen, der häufigen Verwendung und dem vorhandenen Potenzial, in womöglich zukünftig auch kurativen Therapielinien zum Einsatz zu kommen, werden auch Intensivmediziner:innen häufiger mit irAEs nach Checkpointinhibitoren konfrontiert sein. Dementsprechend ist das Verstehen, Erkennen und Therapieren von Nebenwirkungen nach Immuntherapien zunehmend essenziell.
Keywords: Adverse reaction; Checkpoint inhibition; Immune-related adverse events; Immunotherapy; Organ failure.
© 2023. The Author(s).


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
